


ALL PRACTITIONERS have fit a patient in scleral or specialty contact lenses, spending a significant amount of time designing the lenses, providing training, and getting a great fit—but the patient isn’t happy. The patient may complain of eyelid irritation, eyelid sensation with the lenses, fluctuations in vision and transient blur with blinking, deposits on the lens…the list goes on (Figure 1). So, what is the problem?

In my experience, these outcomes usually stem from undiagnosed and undertreated dry eye, meibomian gland dysfunction (MGD), blepharitis, or a combination of all 3. The result is the same—the patient in the chair is frustrated and the practitioners are frustrated they didn’t manage this before it became a problem.
In January, at the 2025 Global Specialty Lens Symposium (GSLS), there was a lecture on the importance of managing the ocular surface and lids in the presence of specialty contact lenses. This topic is crucial to the success of the patient who wears specialty lenses. Specialty lenses can truly cause life-changing outcomes, providing patients with improved quality of life and significantly improving vision, but pesky dry eye can ruin the party.
Specialty contact lens providers have many tools at their disposal to anticipate issues ahead of time, ascertain patient expectations, and choose lens designs that provide the best outcome possible.
At the initial patient visit, consider using a validated questionnaire related to dry eye and the patient’s symptoms. Examples include Contact Lens Dry Eye Questionnaire-8 (CLDEQ-8), Standard Patient Evaluation of Eye Dryness (SPEED), Ocular Surface Disease Index (OSDI), Dry Eye Questionnaire-5 (DEQ-5), and Dry Eye-Related Quality-of-Life Score (DEQS) (Stapleton et al, 2024). Depending on the patient’s contact lens history and their reason for seeking specialty lenses, use the appropriate questionnaire.
Even if the patient is not presenting for specialty lenses related to dry eye, practitioners know the ubiquitous nature of dry eye and its subclassifications (Dossari et al, 2022). Using a survey can help clue the patient in that there is a cause for the symptoms and that steps will be initiated prior to lens wear to help manage them. Patients who are unwilling or unable to successfully and consistently manage concurrent lid disease and dry eye need to be counseled on the impact this could have on their satisfaction and success of specialty lens wear.
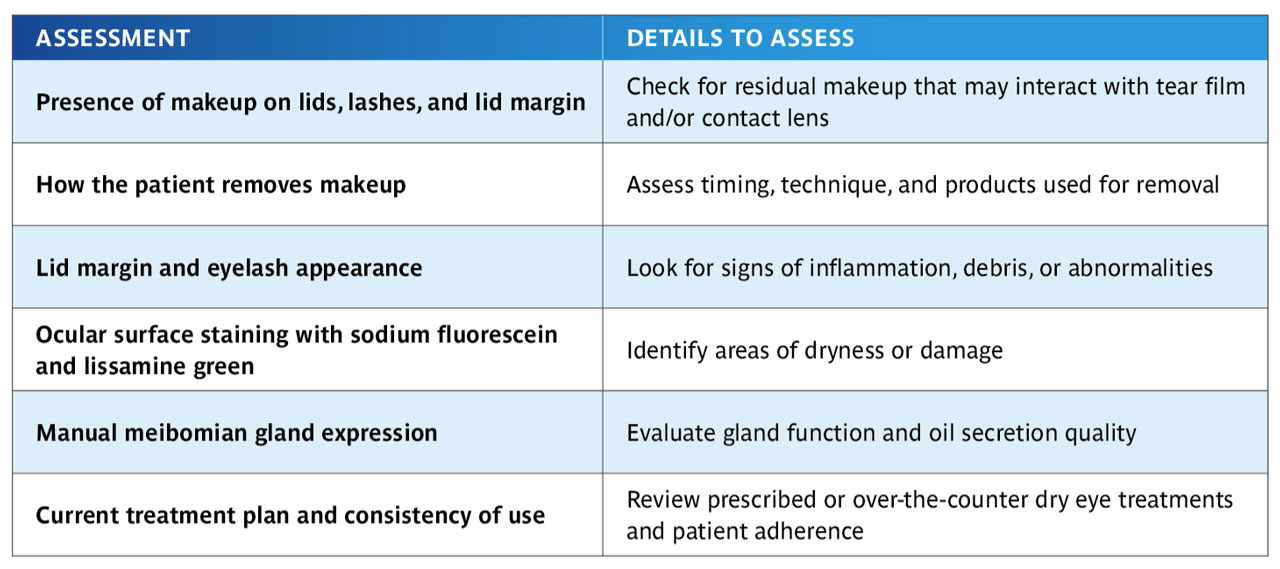
Next, during the initial slit lamp and external exam, specifically document the condition of the lids and ocular surface, the presence of staining, and the meibomian gland function, along with an accurate history (Table 1).
After gathering this information, the practitioner can develop a plan with patients to set them up for success and teach them that specialty contact lenses are not the only tool required to manage complex ocular conditions. It is helpful to provide patients with typed instructions as to what ocular surface treatments they need to start and maintain once they begin wearing specialty lenses.
At the end of the day, the patient and the specialty contact lens provider are a team. Practitioners should set the reasonable expectation that using specialty lenses requires effort, consistency, and the choice of specificity in treatment and products. By doing this work ahead of time, patients can have better outcomes and practitioners can have happier patients.
References
1. Stapleton F, Velez FG, Lau C, Wolffsohn JS. Dry eye disease in the young: A narrative review. Ocul Surf. 2024;31:11-20. doi: 10.1016/j.jtos.2023.12.001
2. Dossari SK, Alkhars AZ, Albaqshi AA, et al. Prevalence of dry eye disease and its risk factors among the general population of saudi arabia: a cross-sectional survey. Cureus. 2022;14(12):e32552. doi: 10.7759/cureus.32552