


THE CONTACT LENS world is constantly evolving. Staying up to date on the latest trends in the contact lens industry is essential for keeping practitioners aware of the advancements that may benefit their patients—and for looking forward to learn what contact lens technology can provide next. The 2025 GP and Custom Soft Annual Report is derived from polling the responses of readers of Contact Lens Spectrum (CLS) and other experts in the industry.
In addition, members of the GP Lens Institute (GPLI) advisory board were asked to offer their thoughts about the current hot topics in the field of contact lenses (GPLI survey). Overall, innovations in scleral lenses were at the top of the list, followed by higher-order aberrations (HOA)/wavefront correction/aberrometry for GP lenses. Myopia management and orthokeratology were also high on the list, and management of presbyopia followed closely.
These trends largely align with the responses to the survey completed by readers of CLS. The CLS reader survey posed questions to practitioners about the use of various specialty lenses in their own practices. Following is a deeper dive into those responses.
GP Lenses
Although most modern lens materials are technically “gas permeable,” this term is often used in reference to lenses that are oxygen permeable and maintain their shape during wear. Rigid GP materials have been recently reported to make up 10% of the contact lenses fit in the United States and 11% of lenses fit internationally in 2024.1,2 These materials are used most commonly in corneal lenses, scleral lenses, hybrid lenses, and orthokeratology lenses.
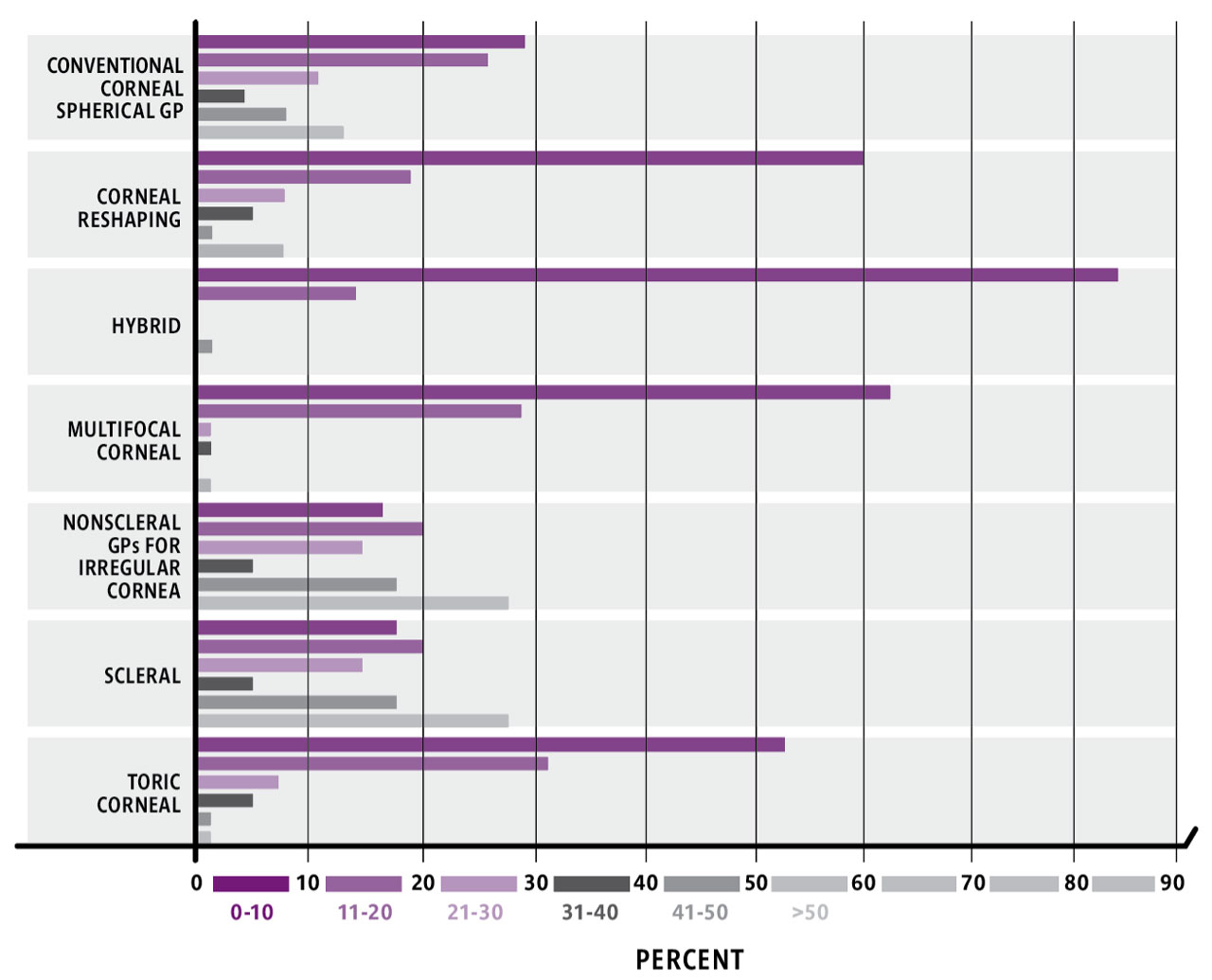
Contact lens materials with increasingly higher levels of oxygen permeability have been developed in recent years. Practitioners are embracing these highly permeable materials among GP lenses in a 2024 survey.1 Readers of CLS who currently fit lenses containing rigid GP materials were asked to report the percentage of various types of lenses in this category (Figure 1).
Scleral Lenses
Members of the GPLI advisory board polled for this article listed advancements in scleral lenses as a hot topic for 2025. This is corroborated by responses to the CLS reader survey: 27% of respondents reported that more than half of their GP lens fits were scleral lenses. Comparing this to respondents to past CLS reader surveys shows an upward trend, with 22% of the respondents in the 2024 survey3 and 13% in the 2023 survey4 reporting that scleral lenses comprised 50% or more of the GP lenses they fit in their practices.
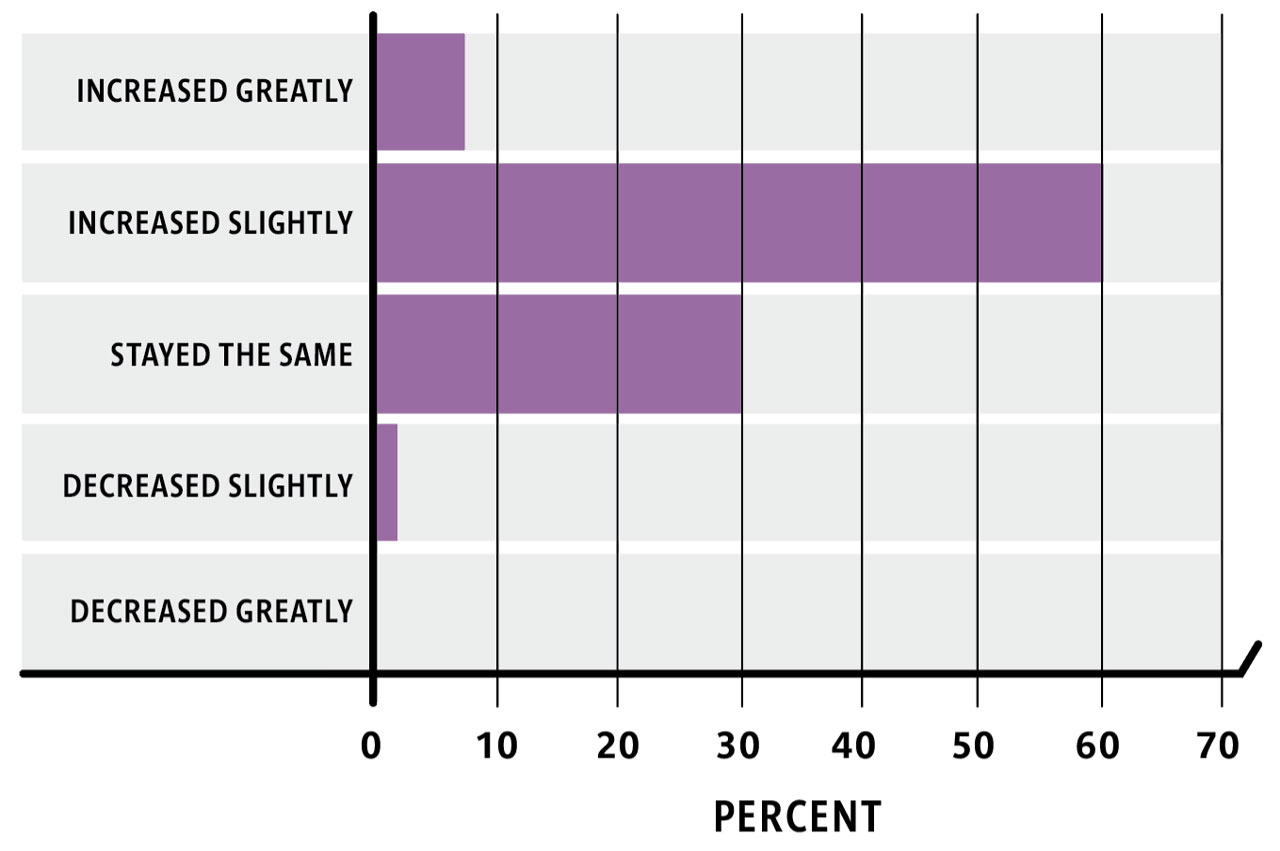
Further evidence of the increase in scleral lens fitting is evident in the CLS reader survey. Sixty-seven percent of respondents reported that scleral lens use had increased in their own practices over the last 12 months (Figure 2). These findings further align with the growth in scleral lens preference found in previous studies examining the practice habits of scleral lens practitioners. In those studies, practitioners who regularly fit scleral lenses preferred fitting corneal GP lenses for corneal irregularity in 2015,5 compared to a greater preference for scleral lenses for the same condition in 2020.6
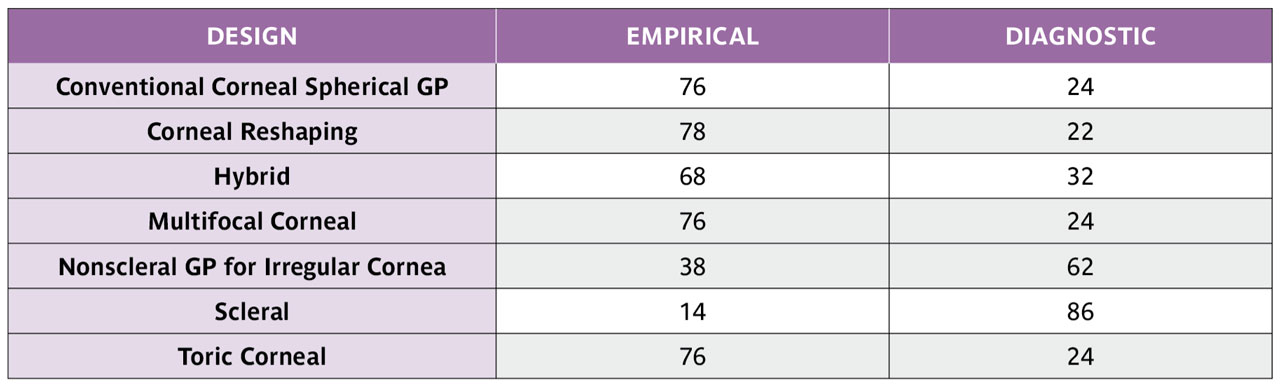
The CLS reader survey showed that 86% of readers reported fitting scleral lenses using diagnostic lenses rather than fitting these lenses empirically (Table 1). Although early GP scleral lens fitting sets primarily used spherical haptic zones, studies have shown that a large proportion of eyes do not have spherical scleral contour.7,8 Diagnostic lens sets are currently available with different types of haptics, or landing zones, to give practitioners the ability to custom fit lenses that match each patient’s unique scleral shape. On average, the CLS survey showed that readers order spherical haptics for 32% of fits, toric haptics for 49% of fits, and quadrant-specific haptics for 30% of scleral lenses.
Thirty-six percent of CLS readers reported using profilometry to aid in scleral lens fitting. This was an increase from 25% in 2024 and 17% in 2023.3,4 The growth in the use of technology in scleral lens fitting is not surprising, given the availability of several devices that can accurately map the ocular contour.9 Practitioners and researchers continue to report using technology both to fit lenses that match ocular contour for fitting purposes,10 and for improving aberrations commonly found in the eyes of patients who wear scleral lenses.11
The GPLI advisory board’s enthusiasm about technology that can measure and design lenses for scleral lens wearers with HOAs is also mirrored in recent scientific literature. Correction of HOAs with rigid lenses is not new, as corneal lenses were shown to reduce aberrations in the past.12 However, the increase in availability of instruments for this purpose has created enthusiasm among scleral lens fitters hoping to help those patients who have acceptable high contrast acuity, but complain of poor vision. Wavefront-guided scleral lens correction is the latest strategy for improving the quality of vision for these patients,13 and developments in this area will likely drive more scleral lens design innovations.
As with all lens modalities, scleral lenses wear is not without challenges, and midday fogging is common among wearers.14 Researchers continue to explore strategies for minimizing the amount of disruption of clear vision from scleral lens wear, although no single fitting methodology or lens/solution property has been found to eliminate fogging for all patients.15 Because midday fogging reportedly has occurred in as many as 58% of habitual scleral lens wearers,16 it is helpful to preemptively explain the likely need for periodic scleral lenses removal and refilling with fresh filling solution during the day.
Corneal Irregularity
The most common indication for scleral lens wear is corneal irregularity.17 The CLS reader survey asked the percentage of patients who had corneal irregularity and were fit with various types of specialty contact lenses (Table 2). Because averaging each category does not result in all categories adding to 100%, comparison of the magnitude of the responses is necessary. When asked specifically about fitting patients with corneal irregularity, readers reported fitting an average of 53% of these patients with scleral lenses. This finding suggests growth compared to a large study in 2020 in which 42% of practitioners reported that scleral lenses were their first choice for fitting irregular corneas.6
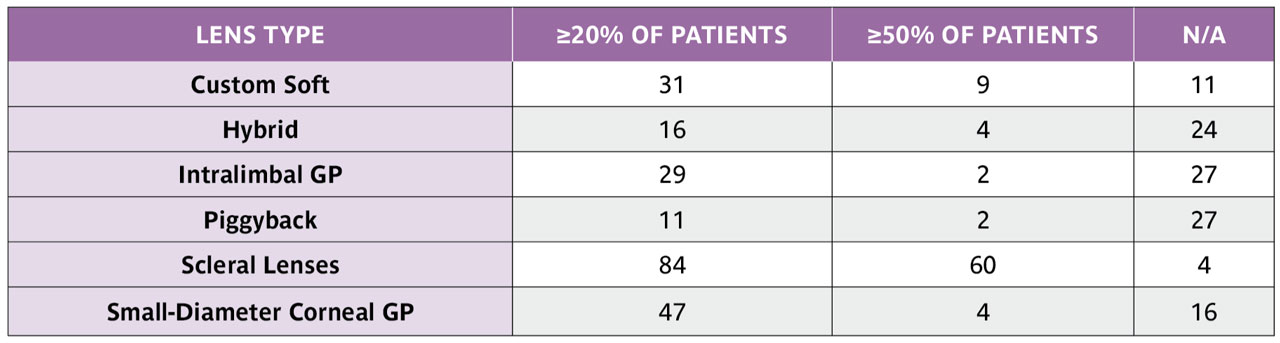
The CLS readers also responded that nonscleral GP lenses were used slightly more often (55%) than scleral fits when combining the categories of small-diameter corneal GP lenses (23%), intralimbal GP lenses (18%), and corneal GP lenses used as part of a piggybacking system (14%). Hybrid lenses were used for corneal irregularity for an average of 15% of fits. In 2025, an average of 20% of practitioners prescribed soft custom lenses for irregular corneas.
It is important to recognize that there is not one specific lens type that will work for all patients who have corneal irregularity. One study of patients who have keratoconus showed similar visual performance among lenses of different sizes and materials, including corneal GP lenses, scleral lenses, and soft and GP lenses designed for keratoconus, concluding that factors including the quality of the lens fit, lens comfort, and the cost of the lenses were more important than what type of lens was fit.18
Corneal GP lenses
Of course, corneal GP lenses can be used for more than corneal irregularity, and these lenses continue to be fit commonly in practice. Corneal GP lenses are also often used for correction of refractive error, particularly for prescriptions not readily available in soft manufactured lens parameters, and for various medically necessary indications, including aphakia and nystagmus.19,20 The ease of handling and the customizable nature of GP lenses also make them an excellent option for patients of all ages, from infants with aphakia to presbyopic patients with discriminating visual demands.
Participants in the CLS reader survey reported that conventional spherical GP contact lenses are fit empirically by the majority of fitters (76%) (Table 1). This was also true for fitting hybrid lenses (68%), multifocal lenses (76%), and toric corneal lenses (76%). Specialty corneal GP contact lenses that are specifically designed for irregular corneas were reportedly fit using diagnostic lenses by the majority of survey respondents (62%).
Astigmatism
Contact lens options abound for patients who have regular astigmatism, with standard soft toric lenses often providing excellent vision for patients who require lower cylinder correction. Patients who have more than 2 D of astigmatism have some standard soft toric lens options, depending on the overall prescription, and also have great options with customizable lenses. Specialty lens fitters know that GP and specialty lenses can provide fantastic acuity for eyes with high astigmatism.
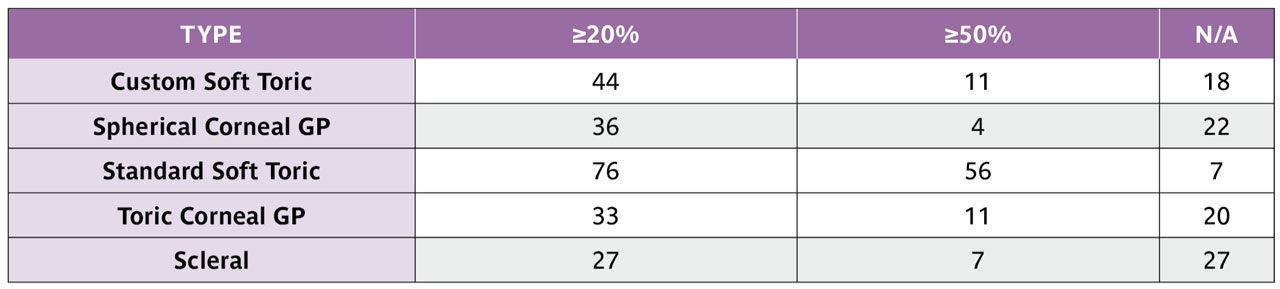
The CLS reader survey asked readers to estimate the percentage of several modalities of lenses that work well for refractive astigmatism greater than 2 D (Table 3). With the current availability of soft toric lenses in higher cylinder powers than previously available, it is no surprise that standard soft toric lenses were used most often by practitioners for this population. Of the specialty lenses available for these patients, the average estimate of custom soft lens usage was 25%, followed by 22% usage of both toric corneal GP lenses and scleral lenses. Spherical GP lenses were estimated to be used in 20% of fits for astigmatism over 2 D.
Orthokeratology
Although GP lenses used for orthokeratology are similar in size and appearance to corneal GP lenses, the reverse-curve profile of the lenses that create the treatment effect of these lenses truly make them worthy of inhabiting their own category. The growing enthusiasm for myopia control has fueled interest in this lens modality.21 Additionally, many adults enjoy the carefree lifestyle that results from wearing these lenses overnight in order to go without vision correction during the day.22 Of the contact lens fitters responding to the CLS reader survey, 48% reported that overnight orthokeratology lens fitting had increased in the past 12 months, with 9% saying that fitting these lenses had increased greatly.
Myopia Control
Although orthokeratology has been used for myopia control for many years, other options have been introduced over the years, providing solutions for patients who do not wish to wear lenses overnight or have prescription or corneal curvatures that aren’t ideal for orthokeratology.23
Low-dose atropine eye drops have been found to slow myopia progression and can be prescribed for all children, regardless of refractive error.24 To date, no formulations of low-dose atropine have been approved by the US Food and Drug Administration (FDA), so these eye drops must be used off label and must be made by compounding laboratories. Studies do not all agree as to what dosage of low-dose atropine is most effective for myopia control.24
Specific designs of soft multifocal contact lenses have been shown to be similarly effective for myopia control, with the Bifocal Lenses In Nearsighted Kids (BLINK) study showing effective myopia control with a distance-center designed multifocal lens with a +2.50 add power.25 A dual focus lens has been FDA approved for children with 4 D of myopia or less.26 Comparison of these myopia control methods do not show a single ideal treatment for all patients, and having options allows for personalized treatment that meets the needs and lifestyle of each child.
Finally, although they are not yet available in the United States, spectacles specifically designed to slow the progression of myopia have been used internationally for several years.27
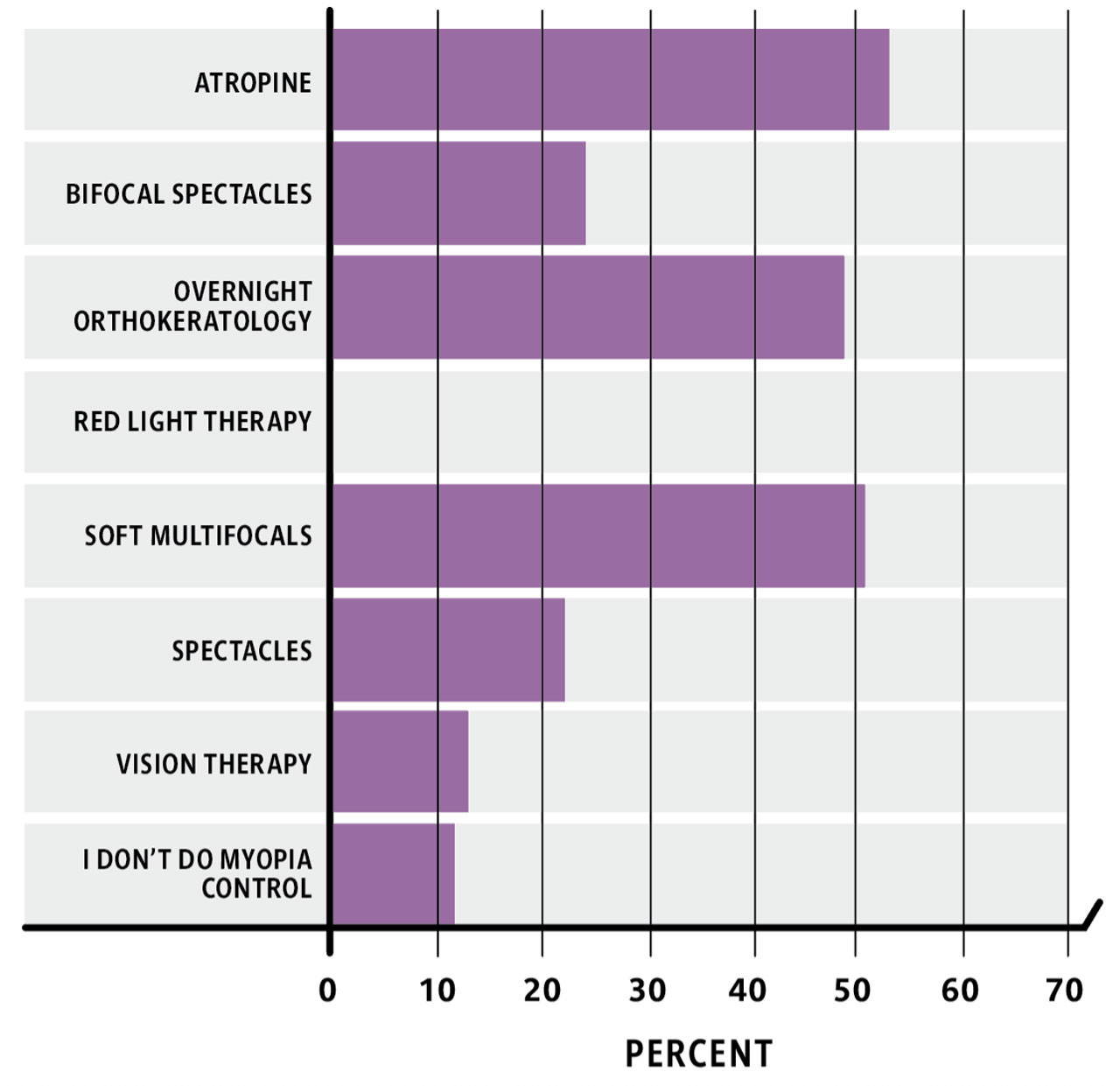
The CLS reader survey posed questions about myopia control treatments used in practice (Figure 3). Of the respondents, 27% said they did not do myopia control. Low-dose atropine was used by the highest percentage of practitioners (53%), followed closely by myopia control soft multifocals (51%) and orthokeratology lenses (49%). Despite the lack of availability of myopia control spectacles in the United States other than sites participating in clinical trials, 22% of those participating in the study reported using these glasses in their practices. This finding may highlight the international readership of CLS.
Presbyopia
Presbyopic patients have more contact lens options than ever before, and fitting these patients in contact lenses—whether with standard soft multifocal lenses or with custom GP lenses—is increasing internationally.28 Practitioners have fewer lens options for those patients who have both presbyopia and astigmatism. The CLS reader survey posed questions on the percentage of lenses fit for patients with both presbyopia and 1 D of refractive astigmatism (Table 4). The lens modality selected most for this scenario was standard soft multifocal contact lenses (45%). Custom soft multifocal lenses were the next most commonly fit option (29%), followed by GP aspheric multifocal lenses (22%), translating GP lenses (21%), and hybrid lenses (17%).
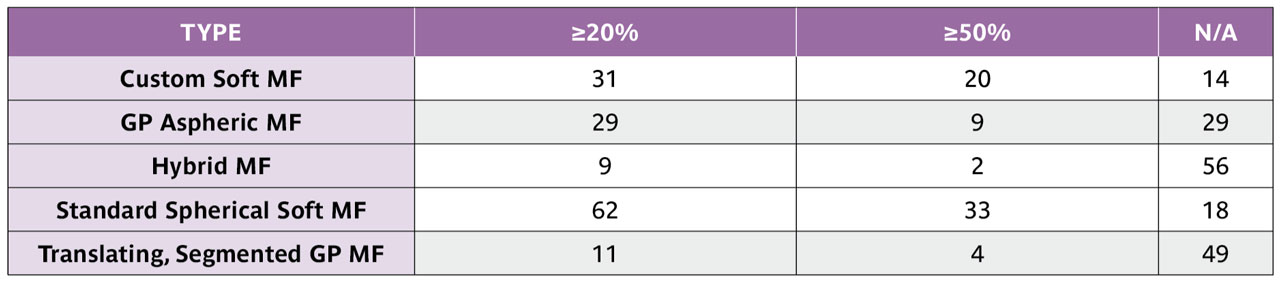
It should be noted that several soft standard multifocal contact lenses are now available with toric correction. These lenses will help soft astigmatic contact lens wearers transition into presbyopia much like their counterparts who only required spherical single-vision lenses before they became presbyopic.
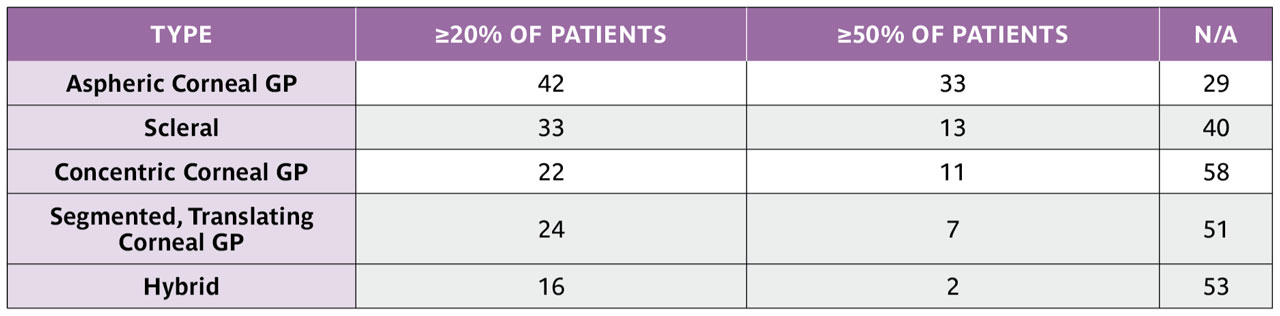
Of course, patients who wear GP and specialty lenses deserve to see near objects clearly when presbyopia occurs, too. Table 5 shows the percentage of lens types being fit for multifocal correction of presbyopia. Thankfully, wearers of GP lenses can be easily transitioned into lenses that correct vision at multiple distances. Laboratories have numerous lens designs available to incorporate add power into lenses.
GP and custom soft lenses have become more popular over the past 10 years.1 The success of scleral lenses and orthokeratology lenses have played a role in this growth, and have likely reminded practitioners of the availability of lens materials and customization that can greatly impact the vision and quality of life for their patients. As contact lens labs continue to innovate, keeping up to date on the lens designs available for all modes of vision correction is an excellent way to make sure patients can achieve the best possible vision.
References
1. Morgan PB, Woods CA, Tranoudis IG, et al. International Contact Lens Prescribing in 2024. Contact Lens Spectrum. 2025;40(1):22-24,26,28-30. clspectrum.com/issues/2025/januaryfebruary/international-contact-lens-prescribing-in-2024
2. Nichols JJ, Fisher D. Contact Lenses 2024. Contact Lens Spectrum. 2025;40(1):12-13,15-16,18-19. clspectrum.com/issues/2025/januaryfebruary/contact-lenses-2024
3. Bennett ES. GP and Custom Soft Annual Report 2024. Contact Lens Spectrum. 2024;39(8):10-12,14,16,32. clspectrum.com/issues/2024/october/gp-and-custom-soft-annual-report-2024
4. Bennett ES. GP and Custom Soft Annual Report 2023. Contact Lens Spectrum. 2023;38(10):24-31. clspectrum.com/issues/2023/october/gp-and-custom-soft-annual-report-2023
5. Shorter E, Harthan J, Nau CB, et al. Scleral lenses in the management of corneal irregularity and ocular surface disease. Eye Contact Lens. 2018;44(6)370-378. doi: 10.1097/ICL.0000000000000436
6. Shorter E, Fogt J, Nau C, Harthan J, Nau A, Schornack M. Prescription habits of scleral lenses for the management of corneal irregularity and ocular surface disease among scleral lens practitioners. Eye Contact Lens. 2023;49(2):46-50. doi: 10.1097/ICL.0000000000000963
7. DeNaeyer G, Sanders DR, van der Worp E, Jedlicka J, Michaud L, Morrison S. Qualitative assessment of scleral shape patterns using a new wide field ocular surface elevation topographer: the sssg study. JCLRS. 2017;1(1):12-22. doi:10.22374/jclrs.v1i1.11
8. van der Worp E, Graf T, Caroline PJ. Exploring beyond the corneal borders. Contact Lens Spectrum. 2010;25(6):26-32. clspectrum.com/issues/2010/june/exploring-beyond-the-corneal-borders
9. Fogt JS, Schornack M, Nau C, Harthan J, Nau A, Shorter E. Image- and impression-based technology in scleral lens fitting for keratoconus: availability and utilization. Eye Contact Lens. 2024;50(7):292-296. doi: 10.1097/ICL.0000000000001100
10. DeNaeyer G, Jedlicka J. Instrument-based scleral lens fitting. Contact Lens Spectrum. 2021;36(11):34-40. clspectrum.com/issues/2021/november/no-fee-ce-instrument-based-scleral-lens-fitting
11. Barone V, Petrini D, Surico PL, et al. Profilometry-guided scleral lenses improve visual acuity and reduce ocular aberrations in irregular corneas: a retrospective case series. Eye Contact Lens. 2025. [Online ahead of print] doi: 10.1097/ICL.0000000000001199
12. Dorronsoro C, Barbero S, Llorente L, Marcos S. On-eye measurement of optical performance of rigid gas permeable contact lenses based on ocular and corneal aberrometry. Optom Vis Sci. 2003;80(2):115-125. doi: 10.1097/00006324-200302000-00007.
13. Marsack JD, Ravikumar A, Nguyen C, et al. Wavefront-guided scleral lens correction in keratoconus. Optom Vis Sci. 2014;91(10):1221-1230. doi: 10.1097/OPX.0000000000000275
14. Bergmanson JP, Walker MK, Johnson LA. Assessing scleral contact lens satisfaction in a keratoconus population. Optom Vis Sci. 2016;93(8):855-860. doi: 10.1097/OPX.0000000000000882
15. Fogt JS, Nau C, Harthan J, et al. Lens and solution properties in patients with and without midday fogging. Ophthalmic Physiol Opt. 2024;44(4):769-773. doi: 10.1111/opo.13293
16. Fogt JS, Schornack M, Nau C, Harthan JS, Nau A, Shorter E. Slit lamp findings in scleral lens wearers with and without subjective fogging. Eye Contact Lens. 2025. [Online ahead of print] doi: 10.1097/ICL.0000000000001204
17. Schornack MM, Fogt J, Nau A, et al. Scleral lens prescription and management practices: Emerging consensus. Cont Lens Anterior Eye. 2021;46(1):101501. doi: 10.1016/j.clae.2021.101501
18. Kumar P, Bandela PK, Bharadwaj SR. Do visual performance and optical quality vary across different contact lens correction modalities in keratoconus? Cont Lens Anterior Eye. 2020;43(6):568-576. doi: 10.1016/j.clae.2020.03.009
19. Russell B, DuBois L, Lynn M, Ward MA, Lambert SR; Infant Aphakia Treatment Study Group. The Infant Aphakia Treatment Study Contact Lens Experience to Age 5 Years. Eye Contact Lens. 2017;43(6):352-357. doi: 10.1097/ICL.0000000000000291
20. Bagheri A, Abbasi H, Tavakoli M, Sheibanizadeh A, Kheiri B, Yazdani S. Effect of rigid gas permeable contact lenses on nystagmus and visual function in hyperopic patients with infantile nystagmus syndrome. Strabismus. 2017;25(1):17-22. doi: 10.1080/09273972.2016.1276939
21. Efron N, Morgan PB, Woods CA, et al. International trends in prescribing contact lenses for myopia control (2011–2024): An update. Cont Lens Anterior Eye. 2025;48(5):102451. doi: 10.1016/j.clae.2025.102451
22. Ren Q, Yang B, Liu L, Cho P. Orthokeratology in adults and effect on quality of life. Cont Lens Anterior Eye. 2023;46(3):101824. doi: 10.1016/j.clae.2023.101824
23. Lawrenson JG, Shah R, Huntjens B, et al. Interventions for myopia control in children: a living systematic review and network meta-analysis. Cochrane Database Syst Rev. 2023;2(2):Cd014758. doi: 10.1002/14651858.CD014758.pub2
24. Maulvi FA, Desai DT, Kalaiselvan P, Shah DO, Willcox MDP. Current and emerging strategies for myopia control: a narrative review of optical, pharmacological, behavioural, and adjunctive therapies. Eye. 2025. [Online ahead of print] doi: 10.1038/s41433-025-03949-1
25. Walline JJ, Walker MK, Mutti DO, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: the BLINK randomized clinical trial. JAMA. 2020;324(6):571-580. doi: 10.1001/jama.2020.10834
26. Chamberlain P, Peixoto-de-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optom Vis Sci. 2019;96(8):556-567. doi: 10.1097/OPX.0000000000001410
27. D’Andrea L, Rinaldi M, Piscopo R, et al. Efficacy of spectacle lenses for myopia control: a meta-analysis of randomised controlled trials. Br J Ophthalmol. 2025. [Online ahead of print] doi: 10.1136/bjo-2025-327629
28. Morgan PB, Efron N, Woods CA, Jones D, Jones L, Nichols JJ. International trends in prescribing multifocal and monovision soft contact lenses to correct presbyopia (2000–2023): an update. Cont Lens Anterior Eye. 2025;48(2):102348. doi: 10.1016/j.clae.2024.102348