


WHEN A NEW ORTHOKERATOLOGY (ortho-k) prescriber begins the fitting process, the primary focus is the central bull’s-eye. If that is observed, the rest of the fit tends to fall to the wayside. Hopefully, the following tips can help student interns, optometry residents, and other new ortho-k enthusiasts advance their skills.
Start by shifting focus away from the center bull’s-eye to the dark areas of the sodium fluorescein (NaFl) pattern. The outermost dark ring is the alignment zone, and designing a lens that is well-aligned with the peripheral cornea creates an effective ortho-k lens. Think of the alignment zone like the landing curves of a scleral lens. Sometimes you can get away with a spherical landing, but you often need toric or even quadrant-specific curves to achieve the desired fit.
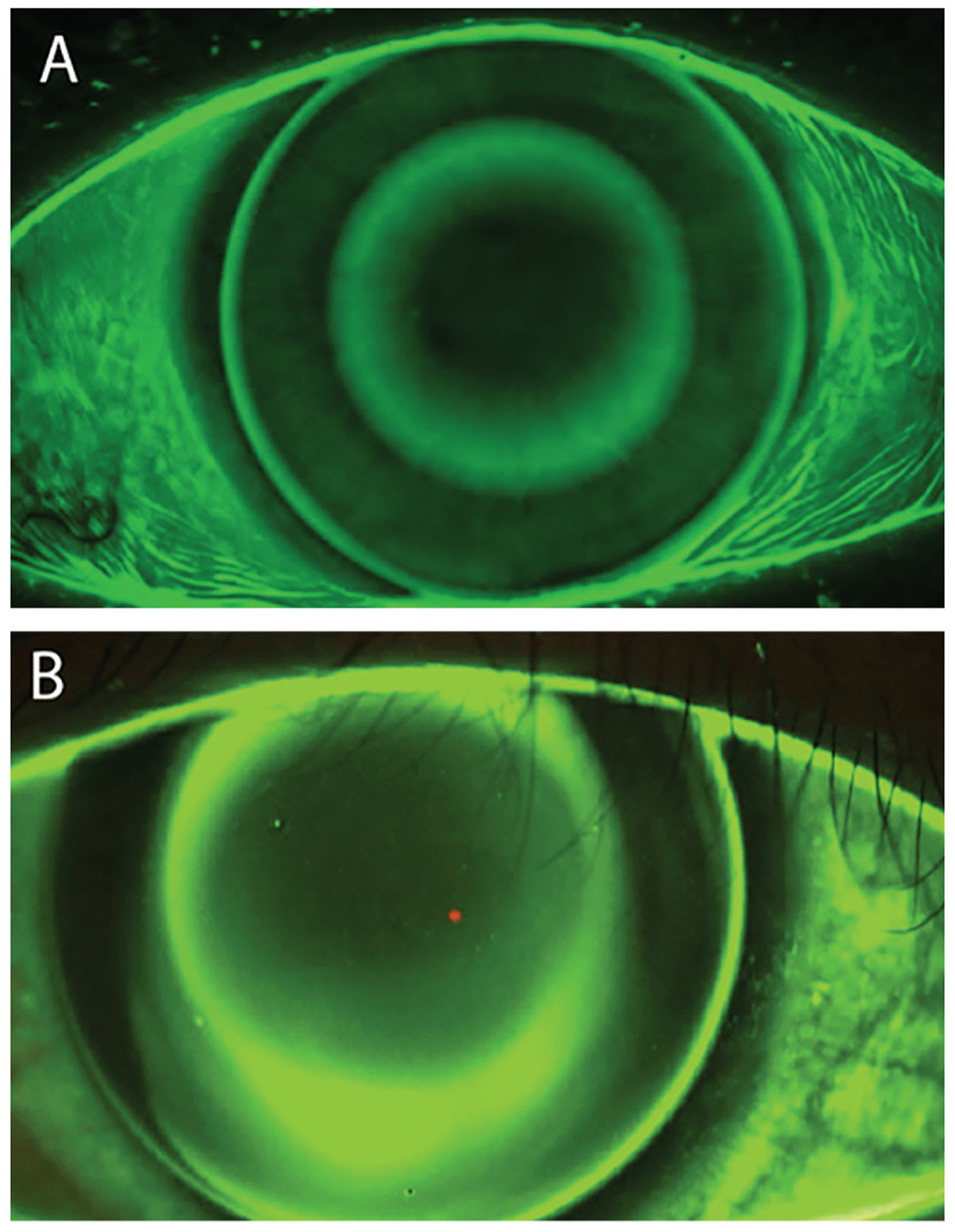
Figure 1A shows an even alignment zone 360° around the center bull’s-eye, whereas Figure 1B shows NaFl bleeding into the inferior quadrant of the alignment zone. The lack of a defined bull’s-eye due to a poor fitting alignment curve can negatively impact the forces that encourage epithelial cell migration. This can lead to decreased acuity or residual refractive error. Similar to scleral lens fitting, adding toric or quadrant-custom peripheral curves can improve the outcome of this process.
While scleral and ortho-k lenses with excessive edge lift can be problematic, so can those with tight-fitting relationships. Ortho-k lenses with alignment curves that are fit too steep to the peripheral cornea can create lens binding that leads to peripheral corneal staining and ocular discomfort. Understanding how the central lens–cornea relationship should look at dispense and follow-up visits can take some time to master. The dark central area of an ortho-k fit should appear defined, but the borders of the surrounding NaFl bull’s-eye will show some tear movement or exchange over the central cornea as the lens moves slightly on blink.
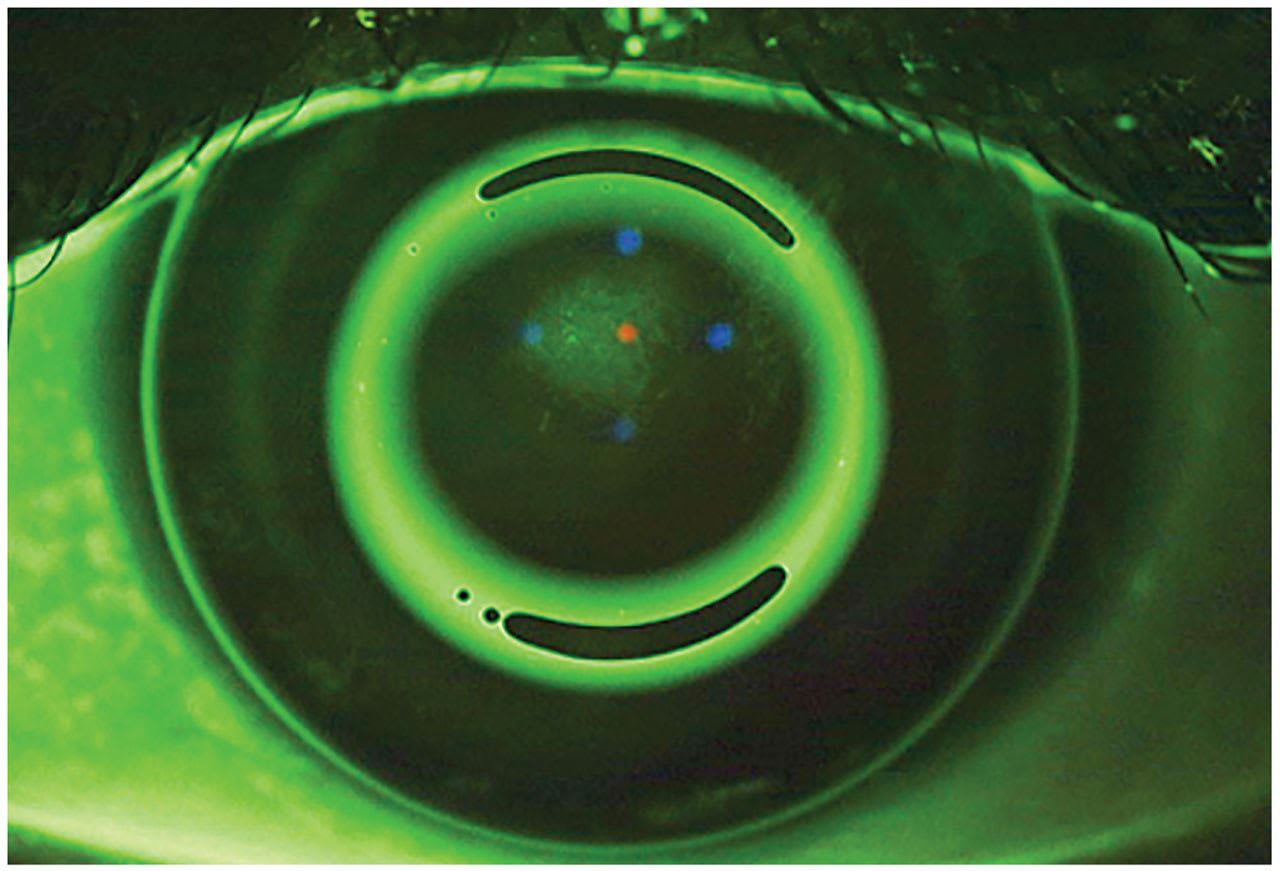
An ortho-k lens that is too shallow will resist exchanging the tear layer over the central cornea and cause central epithelial breakdown (Figure 2). A shallow lens may also show excessive edge lift, as the lens is bearing primarily on the central cornea. When edge lift is present, determine if the lens is too shallow or if the edges are too flat.
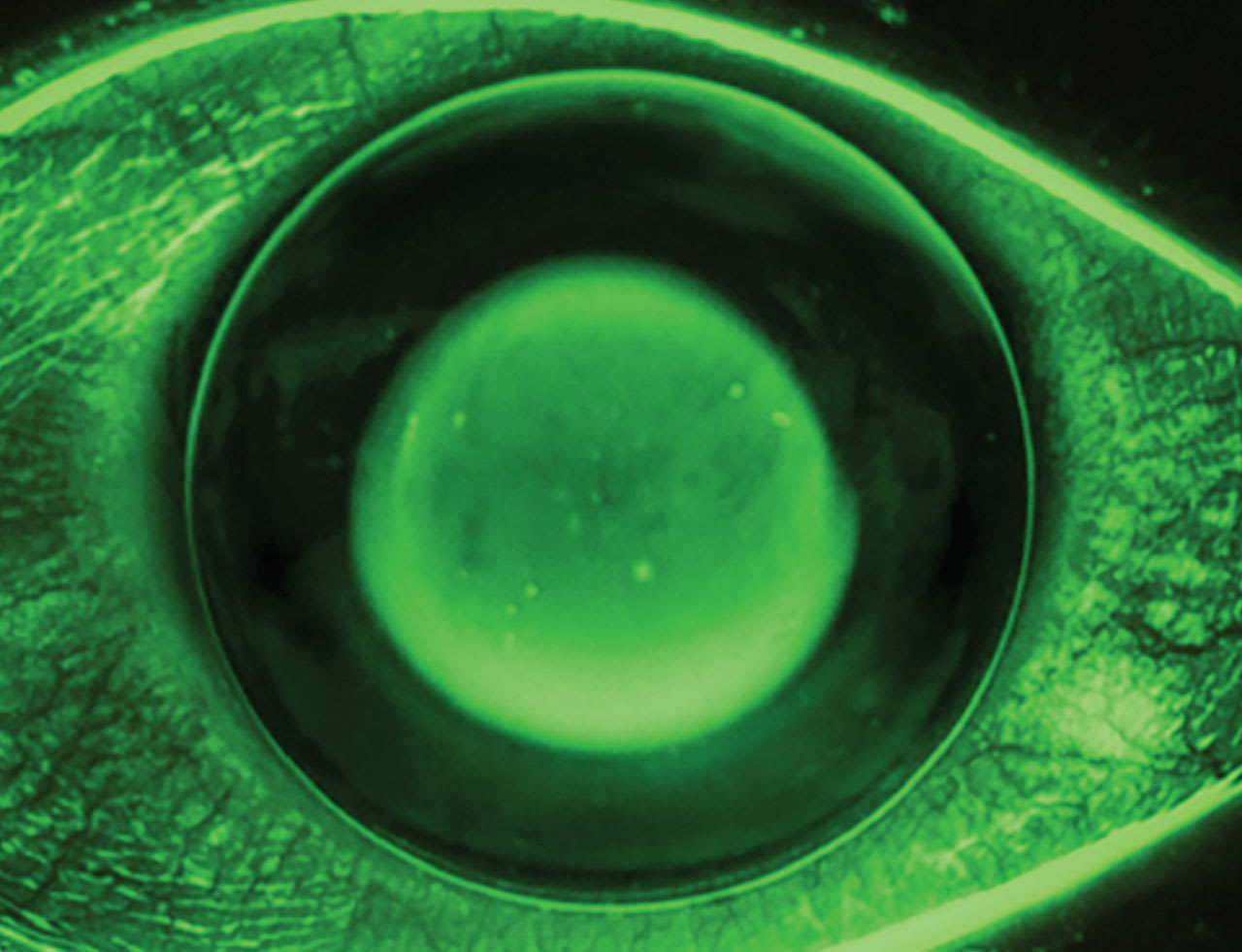
A lens that is too deep will show excess NaFl over the central cornea and is associated with a central island on topography. In this case, the patient will require more minus power in their manifest refraction than anticipated. Although it seems logical to flatten the base curve to correct the residual myopia, the correct remedy is to reduce sagittal depth to properly influence the epithelium. Deep lenses may also decrease tear exchange or show minimal edge lift (Figure 3).
To a new fitter, the bright center bull’s-eye may be the most intriguing part of an ortho-k fit, but one can achieve a stable and predictable outcome by assessing the arguably less flashy peripheral alignment curves.
