


This case describes a patient with significant corneal ectasia and advanced pigmentary dispersion glaucoma with a tube shunt in need of a scleral contact lens.
Case Description
A 53-year-old Caucasian female was referred for a specialty contact lens evaluation by her glaucoma specialist. The patient noted significant blurred vision and monocular ghosting with her glasses. She noted that past specialty contact lenses were unsuccessful due to her glaucoma tube shunt causing contact lens fit issues.
She reported a history of trabeculectomy with tube shunt and cataract surgery 4 years prior. Prior to this surgery, she had reported poor vision due to corneal ectasia. She had worn various types of contact lenses prior to the surgery, but notes after her glaucoma surgery no contact lens was fitting correctly due to the level of her ectasia and the glaucoma tube.
Her entering visual acuity was 20/100 with her glasses and no improvement with pinhole testing was noted. Topography measurements revealed keratometry readings of 45.9/59.7 @175, with a K max of 63.0 D and significant inferior steepening. The glaucoma tube was located superior temporal at the limbus, with an elevation of the conjunctival tissue corresponding to the buried tube.
Discussion
A diagnostic BostonSight SCLERAL lens (BostonSight) was placed in the eye based on the fitting guide with the parameters of 8.00mm base curve and 18.5mm diameter. The initial lens assessment showed adequate fluid reservoir thickness throughout the lens and mild compression in the superior temporal area of the tube shunt. An over-refraction was performed and yielded +5.50 sphere and a visual acuity of 20/20. The patient noted all the ghosting and monocular diplopia she was experiencing in glasses was resolved, with a significant improvement in vision.
Due to the landing over her glaucoma tube, a design modification was made of the quadrant corresponding to the tube location by flattening the scleral lens haptic and adding Smart Channel to accommodate the conjunctival elevation of the tube.
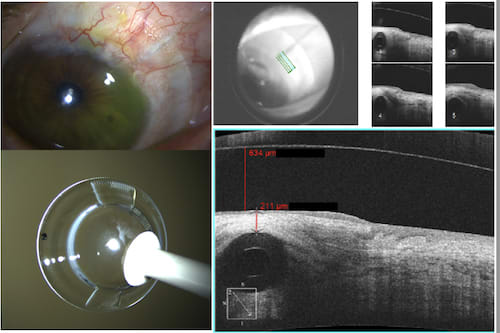
Over the course of her follow-up visits, anterior segment optical coherence tomography (AS-OCT) was used to measure the amount of conjunctival tissue between the tube and the scleral lens to monitor for thinning or excavation of the tube. She has worn this scleral lens design with mild modifications successfully over the course of 3 years without any adverse events or changes in intraocular pressure. She is closely monitored for contact lens follow-ups and by her glaucoma specialist for her underlying disease.
Conclusion
Glaucoma patients in need of specialty contact lenses can be challenging due to the scleral and conjunctival elevation obstacles from prior procedures. With advancing scleral lens design and technology, specific design modifications can be made to aid in challenging cases where glaucoma procedures have induced significant conjunctival obstacles. Close follow-up care, and monitoring of the ocular surface with slit lamp photography and OCT are extremely helpful in cases such as this.
Stephanie Pisano, OD, is a clinical associate professor in the Department of Ophthalmology and Visual Sciences at the Ohio State University Wexner Medical Center in Columbus, Ohio. She discloses an honorarium from BostonSight.