


Multifocal Contact Lenses The Next Generation
Knowing what multifocal designs are available helps you make the best choice for each presbyopic contact lens patient.
BY DAVID W. HANSEN, OD, FAAO
Developments in gas permeable (GP) and multifocal contact lenses often increase success while preserving acuity and stereopsis better than monovision. Take advantage of these improved multifocals and market your expertise to the huge volume of new presbyopes. Critically select the best design for each patient.
Patient selection addresses the four major considerations of motivation, occupation or avocation, the patient's ocular characteristics and the refraction.
Motivation is the key to success. Current lens wearers are slightly better candidates than patients who have never worn contact lenses or spectacles, but a positive motivation of the latter patients can overcome this.
Occupation or avocation of the patient helps determine the type of multifocal. For example, if the computer time exceeds about 35 percent of the day, choose a simultaneous or aspheric design, as they permit smoother intermediate transition from the work task to the computer. Occupations that require an "arm's length" vision range, such as accountants, electricians, mechanics and plumbers, are also excellent candidates for aspheric or simultaneous designs. Patients who have "near to far" demands, such as farmers, teachers and truck drivers, may benefit from a translating design.
Ocular characteristics, when accurately measured, also help determine the most suitable bifocal option. Measure the size and shape of the cornea, eyelid positioning and tonicity, and the pupil size under both mesopic and scotopic conditions. Diagram eyelid positioning. If the lower lid is below the lower limbus, a translating design is usually not recommended.
Corneal topography helps predict the diagnostic lens positioning and provides more successful matching of occupational needs, ocular physical characteristics and appropriate bifocal design. Corneal apex should be close to pupillary mid-point for centering of a simultaneous or aspheric contact lens.
With miotic pupils, aspheric lenses are preferable. Pupils greater than 4.5mm under mesopic conditions contraindicate most bifocal designs because of flare or ghost images. Decreased blink rate patients are poor candidates for any GP lens design, especially translating bifocals. Evaluate the tears for aqueous volume (Zone Quick Test) and tear quality (TBUT or DET tests). A TBUT below 10 seconds usually indicates that all-day wearers of contact lenses will need assistance from punctal plugs.
Examine the corneae, conjunctivae and the limbal junctions, especially for pingueculae, corneal dellen, peripheral corneal hypertrophy, neovascularization, vascular limbal keratitis and dry eye before trial fitting. These conditions decrease probability of success.
Refraction is an important factor in patient selection for bifocal or multifocal contact lenses. Patients with a low ametropia are not generally good candidates. High motivation and new bifocal designs may overcome this.
Fitting GP Bifocal Contact Lenses
If the preselection criteria have been met, the diagnostic evaluation can begin. Use diagnostic contact lenses for all bifocal and multifocal designs. A current wearer of polymethylmethacrylate (PMMA) lenses should first be fitted with GP single vision contact lenses to allow corneal and refractive findings to stabilize, which may take two to three months, before doing the bifocal diagnostic exam. There are a multitude of multifocal designs in materials compatible with the corneal physiology to assist vision from far to near. Bifocal contact lenses are used for pediatric and binocular vision conditions, as well as presbyopia. The goal in fitting a contact lens is to provide convenience, comfort, clarity and tissue integrity. Every patient wants convenience and clear vision as fixation moves from far to near through an intermediate zone without jump.
Multifocal Materials
Bifocals and multifocals are made in GP and hydrogel materials and designs. Silicone hyrodgels will soon follow. Select the appropriate materials for each patient. GP multifocals may have a greater success rate because the optics are easier to customize for individuals. However, the convenience and comfort of disposable and programmed replacement hydrogels provide good reproducible options for many patients. Replacement and duplication of GP multifocals was a significant problem, but technology has alleviated this. Multifocal hydrogels are available in spherical or toric designs, and they are usually made in medium water content materials to assure reasonable oxygen transmission for the thicker toric lenses.
Bifocal Designs
Simultaneous and translating (alternating) designs require different fitting characteristics for success. Carefully understand the patient's visual needs to select the appropriate design.
Simultaneous imagery occurs when a patient sees through the distance and near powers at the same time. The forms of simultaneous lenses include annular or concentric, aspheric and diffractive. The four characteristics of the simultaneous, or "bivision," design are:
- Lenses are usually nonprismatic and require excellent centration.
- Both distance and near refraction are superimposed so the eye and brain try to select light rays most "in focus" for either distance or near.
- Near power is in the periphery or center of the lens.
- Normally these designs lack good intermediate acuity, unless the aspheric design is utilized.
Translating (alternating) lenses also have distance and near power areas. There is usually crisp visual acuity for the two areas. Trifocal designs have three areas for distinct acuity and usually have three characteristics:
- Prism ballast lenses to position the bifocal segment.
- Distance vision usually is produced by the superior and near vision by the inferior region of the lens.
- Depend on the lower lid to hold the lens with downward gaze. Remember that all designs need to translate and move to allow sharp acuity in different areas of gaze.
|
|
|
|
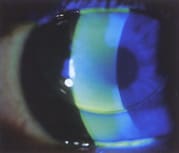
Figure 1. Posterior aspheric GP lens with superior positioning and central
alignment. |
|
GP Simultaneous Designs
The three basic GP simultaneous designs are concentric annular or target, de Carle and aspheric. The first two are non-aspheric and have no prism ballast for orientation. Aspheric designs can have single or multiple posterior aspheric curves with a spherical front surface, or a single posterior aspheric curve with an aspheric anterior surface. These designs offer options for individual advantages (Figure 1).
Target, or concentric annular, designs usually have a front-cut near power and a spherical base curve and have the potential of flare and glare. Excellent centering is necessary to produce the simultaneous effect. Since the front-cut adds can be altered by the cleaning procedures, solution compliance is important. These are fit like a single vision lens and the base curve should provide an even alignment fluorescein pattern. They usually are fit on K or slightly steeper, which depends on the corneal toricity.
Annular (deCarle) designs are back surface annular concave cut add powers that reduce the flare and glare and require a well-centered lens. Unlike the target design, reproducibility and optics are good for distance and near, but lack of an intermediate power area is a negative for computer operators. The non-prism design has the distance 3.0mm to 6.5mm diameter (average diameter is 3.4mm) seg geometrically centered with adds from +1.00D to +3.75D. This lightweight design fits like a single vision lens, and lenticulation is possible. The lens must center on the eye with minimum movement. Patients with large pupils present a problem.
|
|
|
|
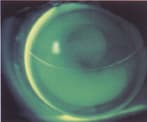
Figure 2. Multifocal aspheric GP lens with inferior positioning. To improve
centration, use a steeper base curve. |

Aspheric progressive designs usually have high eccentricity posterior aspheric and spherical anterior surfaces. A well-centered lens is necessary, and good intermediate visual acuity benefits computer operators (Figure 2).
For most patients, start with an aspheric or simultaneous design. Remember, good centering is needed to produce the simultaneous effect, but flare and glare are always potential problems. Comfort is often good due to the aspheric base curve. Not all aspheric lenses are fit with the same base curve-to-cornea relationship because laboratories use different e-values (eccentricity) to produce the fit and power addition. While the base curves of some designs are 1.50D to 6.00D steeper than K, Boston MultiVision is fit about 0.25D to 0.75D steeper than K because its back surface configuration and creates a +1.50D nominal add. The Essentials is also fit similar to single vision spherical designs. Where centration is difficult, a VFL 3 (Conforma) provides a little intermediate zone flexibility, although centration is still preferred.
Lifestyle Hi-Rider has a back aspheric for fit and front aspheric for power and is fit flatter than other designs to promote slight upward lens decentration and position underneath the upper lid. The base curve is the peripheral fitting zone, called the equivalent base curve (EQBC), rather than the central apical radius of traditional base curves. EQBC is approximately 0.1mm flatter than flat K corneal curvature. Blurred distance acuity indicates need for a slightly steeper EQBC. Overall diameters are 9.0mm and 9.5mm. Near add is enhanced when the upper edge of the lens rides above the superior limbus. Use the 9.0mm diameter unless the patient has a large corneal diameter or palpebral aperture.
Most aspheric lens initial base curves are 2.00D to 4.00D steeper than flat K. The steeper bases are used with greater corneal astigmatism to produce a better lens-to-cornea relationship for the initial diagnostic base curve. Once the lens is on the eye, evaluate the fluorescein pattern, the lens position and visual acuity to help determine the final lens parameters. The VFL 3 lens is usually fit 2.00D steeper than K, the Unilens GP is fit 1.50D steeper than K and the VX GP is fit 4.00D to 5.00D steeper than K. The increase in this steepness relationship increases the amount of add generated by the aspheric curve.
GP Translating Designs
The present seven translating designs each have their own advantages, disadvantages and fitting philosophies: one-piece crescent, Tangent Streak, annular or concentric, decentered de Carle, fused crescent, Solitaire and Presbylite. Knowledge of fitting single vision contact lenses is required as the same concepts are used to select the base curve to provide a good lens-to-cornea relationship. Fit on K and consider corneal astigmatism. Remember the lower eyelid is the support system for lens translation and use of the bifocal segment.
|
|
|
|
Figure 3. Crescent bifocal with segment line properly
positioned. |
|
One-piece crescent. One-piece crescents are a front cut design with spherical base curve, and patients may complain of segment jump and flare and glare from the front cut. One must fit this lens so that the segment is 0.1mm to 0.3mm below the inferior pupillary border (Figure 3).
Tangent Streak. This lens, originally designed by Fused Kontacts, is a one-piece rigid bifocal with a "no jump" design because the seg line between distance and near powers is tangential at the geometric center of the lens. It is available with adds from +0.75D to +4.00D, custom diameters, 1.75D to 4.00D prism ballast and truncation. The bifocal segment can be any height but averages 4.2mm, optics are good and a trifocal is available for intermediate range acuity. The front cut may cause flare and glare at night because of the potential rotation of the lens. The lens is thicker than many other bifocal designs due to the tangent cut on the front surface. The lenses are fit on K or slightly flatter than K as steeper than K fits often results in insufficient translation and excessive lens rotation. With primary fixation, the bifocal segment should position approximately 0.3mm above the inferior pupil margin in mesopic condition, and the lower lens edge should be near the lower lid (Figure 4).
Annular or concentric. Annular or concentric designs also can be considered translating lenses. The Mandell Seamless Bifocal (Con-Cise) is a new alternating design front surface concentric with a central distance area surrounded by a transition area and then the near power. Average diameter is 9.8mm with a 9.6mm to 10.2mm range, and it is fit slightly higher. The distance zone is usually 3.4mm but varies with pupil size and ranges from 3.0mm to 3.8mm. A minus power has a plus lens profile for comfort and ease of translation.
DeCarle. Decentered deCarle lenses have a concave annular design with a prism ballast-decentered superior distance seg. Average seg diameter is 4.0mm, and there is a truncated base of the prism to aid in the lower lid position. The lenses are very reproducible with good optics. The back surface cut reduces the flare and glare problems produced by one-piece designs and also allows for front surface cylinder powers. These designs are usually lighter than other prism ballast designs and available in many different gas permeable materials. Add powers are from +1.00D to +3.75D. This translating design has been very successful. It is usually used when the lower lid is tangent to the limbus, and there is sufficient eyelid tonicity. It also can be used to position a high riding lens or when critical near vision is the major concern.
|
|
|
|
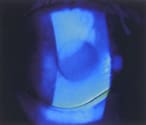
Figure 4. A translating bifocal pulled superior on the eye by the upper
eyelid. |
When troubleshooting the decentered deCarle design, remember that if the segment is too high, reduce the vertical seg height by truncating the lens more. If the seg is too low, order a new lens with a larger vertical diameter. If the lens goes underneath the lower lid, use a thicker lens with more prism and change the design. If acuity is a problem, check the seg alignment or increase the add power.
Fused crescent. The fused crescent translating design was originally created by Dr. George Tseutaki of Fused Kontact Lens Lab in Chicago. This design was available in PMMA material and provided good distance and near visual acuity but poor intermediate acuity. Lens weight was due to the sandwiching of the material. The excellent design was offset by hypoxia from the PMMA material and lens thickness. As the Solution Bifocal (X-Cel) made with GP materials, hypoxia is reduced or eliminated. Plus lenses need less prism and minus lenses more to maintain orientation. Evaluate with trial lens fitting to observe lens position, rotation and translation. The segment is fit below the lower pupillary rim. Truncation may also be used to aid segment position and translation, and truncation should be parallel to the flat segment line with no anterior or posterior taper. It provides good comfort.
Solitaire. This lens is a translating slab-off design with prism and a near portion, which extends across the lower half of the lens, and a monocentric distance seg cut on the superior lens surface. This lens is inherently bottom-heavy because of the removal of weight in the distance area and requires less prism to achieve proper orientation. The segment line should be at, or encroaching upon, the inferior pupillary margin with primary fixation. The fit is similar to other translating GPs, with central alignment and an even fluorescein pattern across the lens.
Presbylite. This lens is a wedge sector translating design from Amsterdam, distributed in the United States, and it has a triangle intermediate zone. A large distance zone allows up to 30 degrees of nasal rotation without diplopia, ghosting or distortion. The untruncated lens is ballasted with 1.5 prism diopters which keeps the lens thin but provides translation from distance to near through an intermediate zone. Presbylite is fit on K or slightly steeper to compensate for corneal astigmatism and to achieve an alignment fluorescein pattern. Lens diameter is usually 9.3mm, but 9.0mm and 9.6mm diameters are available, and the segment is positioned at or slightly above the inferior pupillary margin in normal room illumination. Adds are +1.50D to +3.00D, but don't overplus for near.
Fitting Translating Lenses
Know each lens design and where to position the bifocal segment. For example, fit crescent lens segments near or 1mm below the pupil edge under mesopic conditions, but fit the Tangent Streak segment onto the pupil about 3mm.
Fitting translating bifocals requires the same concepts used with single vision lenses to select the base curve to provide a good lens-to-cornea relationship, such as fitting on K and compensate for corneal astigmatism. The lower eyelid supports the lens for vertical movement to allow the patient to utilize the bifocal segment, and most designs have prism to assist this and to prevent lens rotation.
Soft Multifocals
Soft lens manufacturers have diligently worked to develop multifocal and bifocal designs that provide the crisp visual acuity of GP lenses but without the GP lens movement needed to provide translation from far to near. The comfort of hydrogel lenses combined with disposability provide an expanded array of design modalities, which are usually simultaneous image because of insufficient movement needed for translating designs. Astigmatic correction, however, requires stabile meridional orientation and such designs are available in toric multifocal soft lenses.
Back surface simultaneous aspheric multifocals options usually have limitations at near, but sharper distance visual acuity, while anterior aspheric lenses are the converse. Simultaneous non-aspheric lenses may be the traditional concentric design with the distance power central (centrad) or peripheral (reverse centrad).
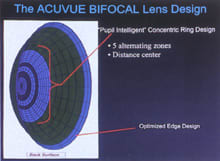
By far the most popular distance-centered soft multifocal is the two-week planned replacement Vistakon Acuvue Bifocal which has a five-ring system to allow clarity for multiple areas of vision (Figure 5). Others in this group include Cooper Frequency 55 Multifocal, Acuity One's Ultra Vue (Figure 6), Lifestyle's Xtra and Specialty Progressive. Near-centered hydrogels include CIBA's Progressives, the Unilens, Westcon Horizon 55 Bi-Con, Abcon N and Ocular Sciences Sunsoft Additions (Profiles A, B and C +2.50D). Gelflex's Triton bifocal lens provides a translating design in a soft lens.
Toric bifocal designs are more limited. Westcon's near-centered toric is the Horizon Toric Bifocal, which is fit with different zone sizes depending on pupil size of the dominant eye. The back surface toric characteristic stabilizes the rotation of the lens that gives the patient stable visual acuity. High add powers can be successfully fit.
|
|
|
|
Figure 5. Schematic of the Acuvue
Bifocal. |
|
Fitting Soft Bifocals
To best fit soft multifocals follow the manufacturers' instructions, fitting guidelines, nomograms and flow charts. Companies often base these on the findings of practitioners who have completed FDA and marketing field studies including development of fitting procedures. Careful consideration has been given to different situations to improve success .
Centration is the key with any hydrogel multifocal. Patients must be able to use the distance and near areas of individual designs, and many patients need to experience different soft lens designs before achieving a successful fit.
"Modified monovision" may supplement soft lens multifocals. A useful rule of thumb is to overcorrect one eye by +0.50D to +0.75D to assist near vision. This modification often turns a marginally happy patient into a successful one. Establish eye dominance or controlling eye preference when using modified monovision techniques. The patient who consistently prefers a controlling eye for distance has a high probability of adapting.
General Fitting Guidelines for All Multifocals
Patients should wear the lenses for about a half hour for adaptation and tear film stabilization. Do not rush this settling period because the lens positioning, movement and translation all aid in the final bifocal success. If you still see excessive movement let the lenses settle for at least another 15 minutes or use other lens parameters.
Over-refract the trial contact lenses and compensate for vertex distances with powers above 4.00D. Use a refractor for the initial power determination by retinoscopy, which helps determine the approximate power for distance and also assesses quality of lens movement and translation. Quickly follow this with a subjective trial lens power assessment, which gives the best power adjustment.
Lens positioning and translation are uniquely tied to lens movement. To raise a low-riding lens, steepen the base curve, or use less prism in a translating design. For a high-riding lens, use more prism in a translating lens, or increase the lens mass by increasing center thickness.
The standard fluorescein evaluation with GPs uses yellow and cobalt filters. Use a Burton lamp for binocular positioning and translation assessment. The biomicroscope is used for subtle lens-corneal monocular relationship measurement. With GP lenses, base curve changes should be in 0.50D (0.10mm) steps to have clinical impact.
Use an in-eye biomicroscope reticule with 10X magnification to determine the seg height, which is measured from the lower lid to the lower pupillary border. To standardize pupil size for bifocal fitting, use a very small slit lamp beam to approximate mesopic illumination.
Compare the over-refraction with the calculated power. If there is much variation, lens position usually needs to be modified. For example, in an aspheric design, if the combination of over-refraction and contact lens power is significantly more minus than expected, the patient is probably looking through the intermediate portion of the lens. Therefore, adjust the lens position to center in front of the pupillary axis.
If the distance seg is too high with translating designs, the lens may be resting on and pushed up by the lower lid. Truncate to lower the distance seg. If the lens is not resting on the lower lid but is being held up by the upper lid, steepen the base curve, increase the prism or reduce the diameter. If the distance seg is too low with translating designs, decrease the prism or order a non-truncated diameter. If the lens rotates nasally, flatten the base curve. If it rotates temporally, steepen the base curve.
With translating or simultaneous designs, if the lens exhibits lateral decentration, it is usually caused by the upper eyelid holding the lens or by a displaced corneal apex. Corneal topography is important to assess the corneal surface. Identify the apex and steepest corneal portions to better understand lens position over the visual axis and to help predict distance acuity. If the lens rides nasally, flatten the base curve. If the lens rides temporally, steepen the base curve.
Manufacturers have excellent consultation services with good support materials. Many laboratories also have patient education pamphlets, practitioner fitting guides and bifocal design calculators to assist in selecting lens parameters. These materials help decide which bifocal designs are more appropriate for each patient's lifestyle and visual needs.
|
|
|
|
Figure 6. Schematic of the Ultravue soft bifocal. |

The literature is now beginning to report high success rates with different designs. These results suggest that bifocal contact lens correction should be considered prior to monovision.
New technology and computerized lathes expand the ranges for most simultaneous lenses. Aspheric curves can be adjusted to accommodate the power for far and near, and aspherics may be the primary choice for some. Patients with residual astigmatism or wide ranges of near visual demands may be best suited for a translating design. Computer usage is a key factor for many when deciding on the initial bifocal design.
The second most important criterion is patient's age. Most translating designs provide higher adds and are better suited to advanced presbyopes. Emerging presbyopes usually do well with simultaneous or aspheric designs, which did not provide enough add power in the past from the aspheric curve to compensate for the visual demands of the aging patients. New designs and improved laboratory technology have solved this. Use aspheric designs or thin translating designs for most new contact lens wearers or whose only experience is with hydrogels.
Conclusion
Fitting GP multifocal lenses requires knowledge about the patient's demands and visual needs. Become involved in this very rewarding specialty area. Small adjustments to base curves and diameters often satisfy the needs of these patients.
Aging is inevitable, as are changes of the crystalline lens, accommodation and presbyopia. Baby Boomers provide an interesting challenge. The contact lens industry has turned its attention to assisting this worldwide population. Is it too late? Have the patients over 45 years given up? I think not!
Dr. Hansen, a diplomate and fellow of the American Academy of Optometry, is in private practice in Des Moines, Iowa.
To obtain references via fax, call (800) 239-4684 and request document #87. (Have a fax number ready.)