


orthokeratology today
Iron Deposition Line
In Ortho-k Patients
BY MARJORIE J. RAH, OD, PHD
We are all aware of the resurgence of orthokeratology, now commonly called contact lens corneal reshaping or corneal refractive therapy. With advances in contact lens designs and materials, this modality is perhaps one of the most exciting options available for our low to moderate myopes. With the recent FDA approval, many practitioners are recommending overnight wear of the lenses.
|
|
|
|
Figure 1. Iron deposition line in
patient wearing reverse geometry lenses overnight. |
|

Iron Deposition Line
Although overnight orthokeratology appears to be safe and effective, an interesting side effect has recently been reported. Brown, circular or arc-shaped deposition, presumed to be iron deposition in the basal layer of the corneal epithelium, has been noted in several cases of patients undergoing treatment with overnight wear of reverse geometry lenses (Figure 1). The location of the iron deposition corresponds to the mid-peripheral steep area seen with corneal topography produced by the secondary curve of the reverse geometry lens (Figure 2).
Similar findings have been reported following refractive sur-gery, which alters the corneal topography in a similar manner to overnight ortho-k with reverse geometry lenses. Likewise, the deposition looks similar to the Fleischer's ring seen in keratoconus patients. Iron deposition is also found in normal patients with no predisposing condition (Hudson-Stahli line), at the anterior head of a pterygium (Stocker's line), near filtering blebs (Ferry's line) and after penetrating keratoplasty. The common link among these conditions and the iron deposition is an abrupt change in corneal curvature and subsequent pooling of tears.
|
|
|
|
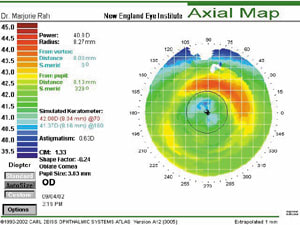
Figure 2. The line's location corresponds to the cornea's mid-peripheral steep
area. |
Deposition Hypotheses
A few hypotheses have been reported to explain the etiology of the iron deposition. One such explanation is that naturally occurring iron in the tear film deposits in the cornea in areas of tear pooling. Another possibility is that iron accumulates in cells in areas of decreased epithelial cell turnover with contact lens wear. The altered geometry of the cornea following ortho-k and the tear pooling in the area under the steep secondary curve of reverse geometry lenses lend credibility to these hypotheses.
Dr. Xie Pei Ying, Peking University Optometry and Ophthalmology Center, spoke on the topic at the Global Orthokeratology Symposium in Toronto. Dr. Ying reported a higher incidence of iron deposition in patients with poor fitting lenses. We have found the deposition to be more easily detected in patients with dark irides and higher baseline refractive errors.
No treatment is necessary for patients presenting with iron deposition as a result of overnight orthokeratology. It appears to be a benign finding that is not sight threatening and does not alter visual acuity.
Dr. Rah is an assistant professor at the New England College of Optometry where she works primarily in the Cornea and Contact Lens Service in patient care, teaching and research.