


treatment plan
Resolving a Soft
Contact Lens Phenomenon
BY WILLIAM L. MILLER, OD, PHD, FAAO
Superior epithelial arcuate lesions (SEALs) are uncommon corneal problems that may prove challenging to manage. An event found only in soft contact lens wear, they can occur in high-and low-water content lenses as well as in lenses worn for either daily or extended wear. Clinicians have reported their occurrence in as low as 0.15 percent or as high as 11 percent of soft contact lens wearers.
First described in the early 1970s, their resurgence of late has come with the emergence of silicone hydrogel contact lenses.
Defining Signs and Symptoms
A patient suffering from a SEAL commonly complains of a mild foreign body sensation much akin to a misplaced ocular surface eyelash. Many times SEALs present unilaterally, but they may also appear bilaterally, although in an asymmetric fashion.
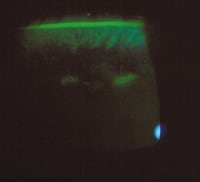
Biomicroscopy will reveal arc-like or horizontal whitish lesions 2mm to 3mm from the corneal limbus, under the upper eyelid. The lesions represent full thickness epithelial breaks, which may form a point of entry for an infiltrative event or eventual subsequent scarring. More readily visible after instillation of sodium fluorescein dye and further enhanced using a yellow barrier filter (Figure 1), SEALs exhibit a delayed streaming (glow) resulting from the disrupted corneal integrity.
|
|
|
|
Figure 1. Instilling fluorescein makes SEALs easier to
detect. |
|
What Causes SEALs?
SEALs may result from many factors, including the higher rigidity of some soft contact lens materials, hypoxia, mechanical chafing, eyelid pressure and poor tear film characteristics. The most likely culprits are mechanical chafing and poor tear film characteristics, with the others presenting as lesser factors.
The combination of mechanical chafing and a poor tear film creates a mechanical force that damages the epithelium and sets up events for an eventual SEAL. You can often detect early mechanical trauma as a subtle linear array of punctate staining in the superior cornea.
Treating SEALs
Treatment options require that patients remove the soft contact lens for three to five days or until the SEAL resolves. This treatment plan will solve nearly one-third of all cases -- even when you refit the patients into the same lens type and material.
Other patients may require a change in material or lens type. You may also need to change to a flatter base curve radius or a soft contact lens design with a thinner edge profile. However, in eight percent to 10 percent of cases this won't prevent the problem from recurring, so you may need to refit the patient into a GP material if he wishes to remain in contact lenses.
Taking Preventive Measures
Increasing ocular lubrication through the use of nonpreserved tear supplements or punctal occlusion may prove useful in cases of presumed SEAL formation, where, as I mentioned earlier, a linear array of punctate staining begins to appear.
Nonpreserved artificial tear supplements and even broad-spectrum topical antibiotics may also prove useful in SEAL cases, with the latter serving as a prophylaxis against any microbial infection.
Dr. Miller is on the faculty at the University of Houston College of Optometry. He is a member of the American Optometric Association and serves on its Journal Review Board. You can reach him at wmiller@uh.edu.