


GP insights
Determining Factors in a Young Patient's Ortho-k Response
BY KRISTIN GLAVINE
Predicting the immediate results of overnight orthokeratology treatment is sometimes difficult. We know that, in general, patients with higher initial prescriptions take longer to achieve full correction compared to patients who begin with lower levels of myopia. Other possible predictors that were investigated, but found to be insignificant, include ocular rigidity, corneal thickness and epithelial fragility.
Here we'll discuss an ortho-k case with an unusual outcome and suggest some factors that might have influenced results.
The Case Study
A 12-year-old African-American female came in for an ortho-k lens fitting as part of a research study. Because of the study's nature, every appointment was scheduled at the same time of day. The patient was scheduled for 3 p.m., although one-day follow-up visits are generally best done early in the morning.
Her entering refractive error was –2.25D OU (20/15) and K readings were 43.25/42.50 @ 008 and 43.25/42.50 @ 010. We fit her with Contex OK E lenses (Contex, Inc.) in Boston Equalens II (Bausch & Lomb) material. The fit was satisfactory, not ideal. The lenses sat slightly inferiorly OU with eyes open but centered upon eye closure. We dispensed the lenses and asked her to return the next day.
She returned the next afternoon for her follow up. Uncorrected entering visual acuities were 20/25-2 OD and 20/15 OS. Her refraction was –0.25D OU (20/15). K readings were 42.75/41.87 @ 162 OD and 42.50/41.62 @ 018 OS. Her topography maps showed a moderate ortho-k bulls eye pattern OU. Figure 1 shows a comparison between the patient's baseline and one-day topography patterns.
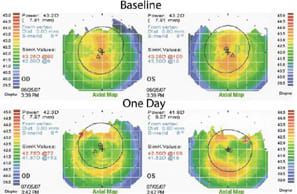
Figure 1. A comparison between the patient's baseline and one-day topography patterns.
An Atypical Outcome
These results aren't typical for ortho-k. In general, a patient beginning at a –2.25D refractive error could take three to five days on average to achieve full correction. CM achieved almost complete correction in one night. Her topography map is also atypical. By 3 p.m. most patients would regress to the baseline pattern with no appreciable bulls eye.
What contributed to these results? Possible factors are age and corneal rigidity. We've noted that children tend to progress faster than adults do with ortho-k. This difference is slight (a day or two).
Corneal rigidity may also be a factor and relates to age differences. Children's corneas may be more malleable than adult corneas. It's possible that a less rigid cornea molds more easily to the ortho-k lens shape.
We're currently investigating corneal rigidity as a predictive factor in the progress of ortho-k treatment. We're using the Reichert Ocular Response Analyzer (Reichert, Inc.) to measure corneal resistance factor (CRF). We hypothesize that patients with lower CRFs will progress faster with ortho-k treatment than will patients with higher CRF values. We're also considering other factors including age and corneal hysteresis, another measurement we can obtain with the ORA. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #142.
Ms. Glavine is a third year OD/MS student at the New England College of Optometry. She is currently working with Marjorie Rah, OD, PhD, in contact lens research.