


FITTING MULTIFOCALS
Fitting Soft Center-Near Design Multifocal Lenses
Following a few simple rules can increase fitting confidence and improve patient success.
By Jill Woods, BSc(Hons), MCOptom; Craig A. Woods, PhD, FAAO; & Desmond Fonn, MOptom, FAAO

Jill Woods is a clinical scientist at the Centre for Contact Lens Research, School of Optometry, University of Waterloo, Ontario, Canada. 
Dr. Craig Woods is the research manager at the Centre for Contact Lens Research, School of Optometry, University of Waterloo, Ontario, Canada. Dr. Fonn is professor and director of the Centre for Contact Lens Research at the University of Waterloo School of Optometry. |
The recent launch of the Air Optix Aqua Multifocal lens (Ciba Vision) means that there are three silicone hydrogel (SiHy) multifocal lenses available. The benefits of SiHy materials have been well documented (Dumbleton, 2006), but until recently they weren't available in multifocal designs. With an aging population, it's likely that a large number of contact lens wearers are approaching presbyopia, which will result in a dramatic increase in demand for multifocal lenses.
The PureVision Multi-Focal (Bausch + Lomb) was launched in 2006. The Air Optix Aqua Multifocal was launched in Europe in January 2009 and in the United States in early 2010. Acuvue Oasys for Presbyopia (Vistakon) was launched in the United States in May 2009. The major parameters of each of these lenses are listed in Table 1.

All three lens designs appear to introduce novel aspects to correct presbyopia that should spark increased interest in fitting presbyopic patients with this modality.
Practitioners are often still reticent to use multifocals as a first choice presbyopic correction (Bennett, 2008), choosing monovision in many cases for their existing contact lens wearers. Thus, it's reasonable to assume that spectacle wearers approaching presbyopia are rarely offered a presbyopic contact lens correction.
The new offerings in silicone hydrogel materials are updated designs and they offer an array of parameters to fit to patients.
All three SiHy multifocal lenses employ a version of aspheric optics in center-near designs. The balance between distance and near in the design varies among manufacturer and also among add powers.
Fitting Guides
Each manufacturer offers its own detailed fitting guide, aimed at improving success rates and removing the confusion that may exist for practitioners not familiar with multifocal contact lens fitting. In this article, we'll describe a generic approach to optimize the optical correction that, when used with the manufacturers' fitting guides, aims to provide increased confidence when fitting multifocal soft contact lenses. This guide was developed at the Centre for Contact Lens Research, Waterloo, Canada, and was derived from the experiences gained over several years of fitting the newer multifocal designs in research trials conducted at the center.
Counsel the Patient
It should be made clear to patients that the multifocal contact lens being fitted won't provide the “perfect” visual solution. Advise patients that just as spectacles don't provide the perfect solution, neither do multifocal contact lenses. The final choice of vision correction will be based on which modality works best for an individual's lifestyle and visual demands. It's important that patients understand that our goal is to find a solution that meets their specific visual demands and fits their lifestyles.
Start at the Beginning
To improve success rates with fitting multifocal contact lens designs, you may find it helpful to adopt the following “R-I-S-O-N-S” to fit multifocal contact lenses.
- R refract
- I initial trial lenses chosen based on refraction
- S settling time of at least 15 minutes before checking acuities
- O over-refract using a trial frame and a fogging technique; avoid the phoropter
- N near assessment
- S send away for a four-day-plus extended trial
- Refract Choose the power of the initial trial lenses from a new refraction rather than from the habitual contact lens powers worn. The refraction should be balanced appropriately and the reading addition determined for the patients' habitual working distance, allowing a range of clear focus—both slightly closer and slightly further away.
The material of the multifocal lens may be different from the lens worn habitually. The multifocal lens prescription therefore will likely be different from that of the habitual lens because of this change in material (Woods et al, 2006) and also because the multifocal lens has a very different design.
At this point, determine the dominant eye for distance. The two most commonly used methods of determining dominance are the “hole in the card” type tests and the blur acceptance test (Collins et al, 1994; Erickson et al, 1992).
Initial Trial Lens Choice Base the initial trial lens power choice on the refraction, taking into account vertex distances and cylindrical power when necessary. Make the choice of reading addition in conjunction with the manufacturer's guide because they all differ slightly.
Settling Time Generally, we found 15 to 20 minutes was sufficient for the lenses to stabilize and for the vision to settle enough to conduct the over-refraction. During this time, allow patients to wander outside of the consulting room as this lets them try the lenses in a less artificial environment and can be beneficial for them to confirm or modify their initial opinions about their vision.
Over-refraction The first step is to determine the distance part of the prescription. For this, use a trial frame with full aperture lenses rather than a phoropter. This helps to keep the visual environment, binocularity, and pupil size as close to normal as possible. Also, the opposing eye should be fogged with +0.75DS or +1.00DS rather than occluded. Check the fogging level to ensure that the acuity is indeed fogged by two lines before commencing.
Start by adding plus power in steps of 0.25D while viewing the distance letter chart. If 0.25D is accepted, then add this to the trial frame and continue until there is a drop in acuity. Check for both plus and minus 0.25D over-refraction, but take care to only add minus if more letters become readable. Resist adding more minus when the patient reports “that seems clearer.” Avoid chasing changes in contrast. We've found that 0.25D flippers are useful for this step, and many manufacturers provide them. Repeat this process with the second eye. Finally, repeat the ±0.25D checking with the patient viewing the chart binocularly—presenting the flippers across both eyes simultaneously and still resisting adding more minus.
If the change to the lens power was greater than 0.50D, apply a new powered diagnostic lens and allow 15 minutes settling before repeating the over-refraction a second time. Getting the distance prescription optimized is the key first step to success.
Near Assessment Only when the distance powers are finalized should the near acuity be measured, as small changes to the distance powers can have a large influence.
Measure the near acuity under binocular conditions, and if it's close to the acuity expected, don't assess any further. Simply proceed to a trial wearing period.
If near acuity isn't as good as expected, then measure acuity monocularly by occluding each eye in turn. Then determine the over-refraction required to attain acceptable near acuity, again using 0.25D steps.
If the near addition of the contact lens seems insufficient, refer to the manufacturer's fitting guide on troubleshooting. Potential solutions include: increasing the plus (or reducing the minus) in the non dominant eye while leaving the add unchanged; changing to a higher add power in the nondominant eye (trying unequal adds); changing from unequal adds to bilateral higher adds.
Send for an Extended Lens Trial When the final power is decided, the real trial of the multifocal modality can begin. It's been shown that a trial over a number of days (four days at least) is preferable to a trial over a number of hours (Papas et al, 2009). An extended trial period should be conducted with the correct trial lens powers as determined using the above described steps. Even if the change was only 0.25D, this can have an impact on patients' perceptions of success, so be sure to send them away in the correctly powered lenses.
A number of studies have compared the performance of monovision to multifocal lenses and have shown that despite similar or slightly worse visual acuity assessments, patient preference for multifocal lenses is high compared to monovision when they're worn in real-life situations (Situ et al, 2009; Richdale et al, 2006).
Don't Multifocals Take Longer to Fit?
There appears to be a perception among many practitioners that multifocal contact lens designs require a longer chair time to fit (Bennett, 2008).
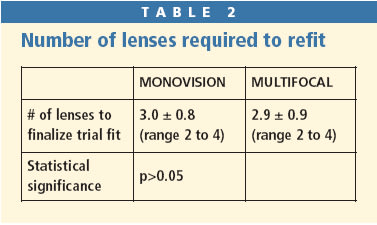
In a recent study by Woods et al (2009), 26 participants requiring their first presbyopic correction were fitted with both monovision and multifocal lenses following a refraction. The number of lenses required to achieve the “walk out of the door” week-long trial fitting was recorded. This number was believed to provide an insight into the chair time required to complete the fitting to this stage. Table 2 presents the results, which show there's no significant statistical or clinical difference in the fitting time between monovision and multifocal lenses. This result may have been influenced by the new lens design used in the study and also by the fact that the participants required a low reading addition.
Satisfy Your Presbyopic Patients
The baby boomers have reached presbyopia and are knocking on our doors, demanding the best technology to keep them active and flexible in their work place and social activities. There are three contact lens options to provide a presbyopic correction together with the benefits of silicone hydrogel materials. When you fit these patients, remember to follow the RISONS Rules. CLS
For references, please visit www.clspectrum.com/references.asp and click on document #172.