


Reader and Industry Forum
Using OCT for Evaluating Complex Contact Lenses
BY JEFFREY SONSINO, OD, FAAO

Successfully managing patients who have irregular corneas with contact lenses can sometimes be a frustrating process for both patients and practitioners. The fitting and evaluation process involves numerous visits to our offices and out-of-pocket expenses for patients, not to mention that practitioners have to deal with the hassle of billing medical and vision insurances.
Luckily, the contact lens industry has responded to our need for better contact lens materials for patients who have complex corneas. It used to be that the only contact lenses available to manage irregular corneas were corneal GP lenses. Now, more and more patients are being fit with newer-generation hybrid lenses and scleral lenses. These newer lens designs are intended to vault over the central cornea and do not contact the central cornea at all. Such contact lenses have resulted in much more comfortable and wearable strategies for full-time use.
Evaluating Newer Lens Designs
With these newer contact lens designs, the game has changed when it comes to the science of fitting and evaluating these lenses. For years, practitioners have used corneal topography to guide their decision-making on fitting irregular corneas. Corneal topography is still an absolutely mandatory part of this process; in keratoconus, for example, it is needed to evaluate the shape of the cone, the simulated corneal curvature, and for monitoring for progression of the disease. It’s important to note that topography is not a standard part of a typical eye examination, as some medical insurances would like us to believe.
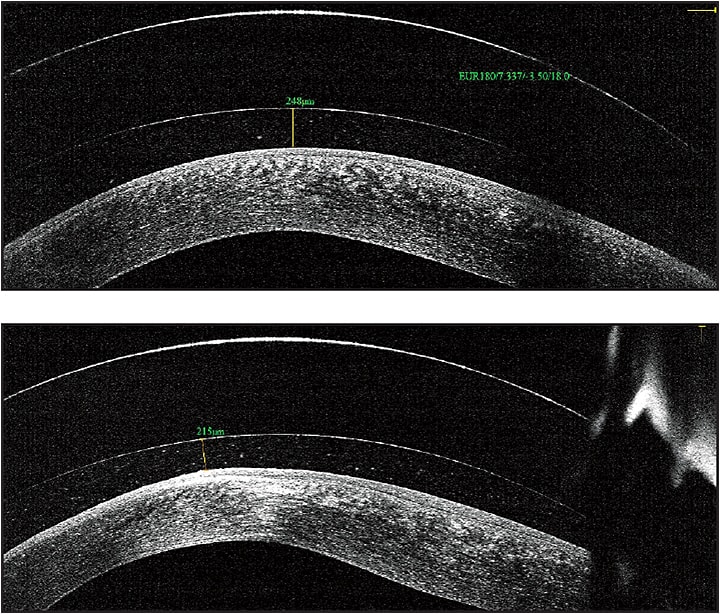
Figure 1. OCT image of a scleral lens fit on a patient who has keratoconus, horizontal line scan (top) and vertical line scan (bottom). The cornea is the opaque white band located at the bottom of each picture, the tear film reservoir is the middle clear band, and the contact lens is the top band. Using an electronic caliper tool, the precise amount of vault can be measured, leaving no doubt as to the precision of the fit.
However, studies show that we cannot use corneal topography to predict the initial trial lenses for scleral contact lens fitting (Schornack and Patel, 2010; Sonsino and Mathe, 2013). Thankfully, we now have another tool at our disposal for evaluating contact lenses on patients who have irregular corneas: optical coherence tomography (OCT).
OCT was once reserved for use in the retina. OCT uses near infrared light passed through the clear structures of the eye to generate a cross-sectional image of the layers of the retina, much like an image generated by magnetic resonance imaging. Advances in OCT technology have improved the resolution to image the eye down to the micrometer (one one-thousandth of a millimeter) scale.
OCT technology is now commercially available not only for the retina, but for the anterior segment as well. The obvious application is to help practitioners with fitting and evaluating complex contact lenses that vault the cornea. Gemoules (2008) was the first to describe a method of using OCT to fit scleral lenses in the literature.
Anterior segment OCT (AS-OCT) allows practitioners to view a cross-sectional image of a contact lens on the eye in real time and to monitor the health of the cornea in the presence of the contact lens. This view is valuable for judging the vault of new contact lens designs over the cornea and for judging where the lenses land on the eye. It is the most specific way to determine whether the lens fit is acceptable and to troubleshoot when the lenses are not fitting appropriately.
AS-OCT gives practitioners a much more powerful tool for evaluating and managing even the most challenging contact lens fits. It remains to be seen whether this technology has the ability to reduce the number of visits required for a successful fit. That said, the precision afforded by this technology can help improve practitioners’ ability to judge what lens changes need to be made to achieve the best fit quickly.
Purchasing an optical coherence tomographer is not an insignificant practice expense. However, models that are equipped to evaluate both the anterior and the posterior segment can make the cost more justifiable.
Billing Pearls When Fitting Complex Contact Lenses
While fitting complex contact lenses can be very rewarding for both patients and practitioners, getting properly reimbursed for these extra services can be frustrating. Following are some tips to help with billing for these difficult contact lens fits:
• AS-OCT (92132) is a billable procedure for use in contact lens evaluations for some medical insurances, but it is considered an experimental procedure to others. There are, however, a number of exceptions to the experimental status. One is “evaluating and planning treatment for patients with diseases affecting the cornea, iris, lens or other anterior segment structures.”
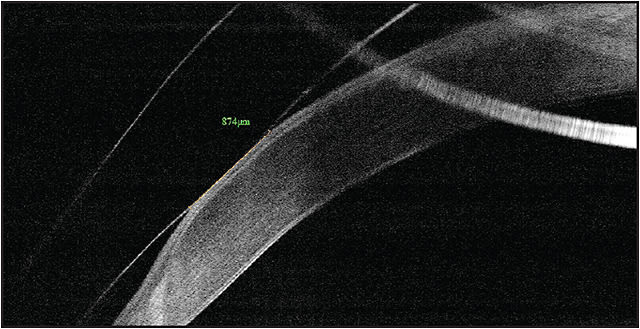
Figure 2. OCT image of the periphery of a scleral lens on a patient who has pellucid marginal degeneration. The lens contacts the cornea over an area 0.87mm long. These types of measurements help guide decision-making in modifying the lens fit and were impossible before the advent of this technology.
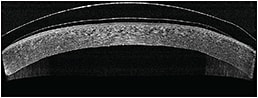
Figure 3. Hybrid contact lens on a highly oblate eye after corneal transplant. The hybrid lens is designed specifically for oblate corneas and lands gently on the peripheral tissue.
In our practice, if we find that a particular insurer excludes this procedure, we write a letter to the plan’s medical director citing evidence in the literature that 92132 is an emerging standard of care and is not experimental. We also cite the 1999 American Medical Association definition of medical necessity and explain why this procedure is medically necessary.
• We ask all complex contact lens patients to sign an Advance Beneficiary Notification (ABN) that explicitly states that all testing and the contact lens materials may not be covered by their medical insurances. The standard Medicare ABN is sufficient. Then, in the examination room, we discuss the importance of AS-OCT and that they may need to pay out of pocket for the procedure if their medical insurance does not cover it. When shown the images, most patients understand why this technology is elevating their care.
• AS-OCT, when used, should be a part of your fee for 92072 (fitting and evaluation of lenses for keratoconus) when submitting to vision insurances (Vision Service Plan and EyeMed).
• 92133 (optic nerve OCT) and 92134 (retinal OCT) are fully reimbursable by most medical insurances.
• Corneal topography (92025) has recently been falsely considered by a few medical insurances to be included in the comprehensive eye examination, similar to keratometry. Bill for this separately, and make sure that you are receiving proper reimbursement. CLS
To obtain references for this article, please visit www.clspectrum.com/references.asp and click on document #233.
Dr. Sonsino is in private practice in Nashville, Tenn. He is a diplomate in the Cornea, Contact Lenses, and Refractive Technologies section of the American Academy of Optometry (AAO). He is also a member of the American Optometric Association’s (AOA) Council on Cornea and Contact Lenses, a fellow of the Scleral Lens Education Society, and is on the advisory board of the GPLI. He is a consultant or advisor to Alcon, Optovue, SynergEyes, and Visionary Optics, and he has proprietary interest in LVR Technology.