



Often, patients who have corneal irregularity and who need a specialty contact lens to achieve improved vision have other comorbidities that can complicate their contact lens fitting. A common example includes patients who have undergone a corneal transplant and have glaucoma; a corneal transplant increases their risk of glaucoma (Kornman and Gedde,2016). Trabeculectomy or shunt surgeries are necessary for patients who have severe glaucoma or poor control of their glaucoma despite maximum medical therapy. These surgeries result in superiorly located bulbar conjunctival blebs that can interfere with contact lens fitting.
If a scleral contact lens is necessary for an eye that has a conjunctival bleb, then a bypass is needed to prevent fitting complications and trauma to the bleb. A beveled notch in the landing zone is an option, especially for patients who have extremely elevated blebs or a bleb that hangs over the limbus. Such patients might also be best fit with a corneal GP lens (Figure 1). The use of localized vaults (Figure 2) has also become increasingly popular. Consider these two critical aspects when using this design approach.

First, the sagittal depth of the localized vault has to be at least equal to the height of the bleb to avoid compression. Additionally, the scleral lens has to be rotationally stabilized to keep the vault in its correct position.
When using spherical landing zones, incorporate a ballasted design. For eyes that have toric or asymmetric scleral shapes, back-surface toric, quadrant-specific, or free-form customized landing zones can be used to lock the lens in its correct rotational position. Patients will have to apply the lens so that the elevation matches the position of the bleb.
Case Example
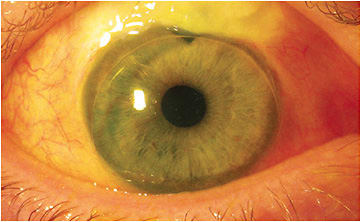
A 70-year-old patient post-penetrating corneal transplant and trabeculectomy for severe glaucoma, who had significant field loss of his right eye, had glasses with a best-corrected visual acuity of 20/100. A slit lamp exam and corneo-scleral topography indicated a flat irregular graft and a superiorly located conjunctival bleb that was distal to the limbus.
A 16.5mm free-form custom scleral lens that included a localized vault was designed from corneo-scleral topography. The lens vaulted the cornea and conjunctival bleb without compression (Figure 3) and improved his vision to 20/50.

Follow Up
It is critical to co-manage these patients with their glaucoma specialist. Additionally, more frequent follow up is necessary at the beginning to monitor the health of the bleb and to ensure that the lens is not mechanically traumatizing the conjunctival tissue or causing an increase in intraocular pressure. CLS
For references, please visit www.clspectrum.com/references and click on document #290.